1 INTRODUÇÃO Ataxia é um termo que literalmente significa ...

of 12
Upload
gabriela-de-aguiar-kufnerCategory
view
231download
08/12/2019 Ataxia Em Gatos
1/12
http://jfm.sagepub.com/Journal of Feline Medicine and Surgery
http://jfm.sagepub.com/content/11/5/349Theonline version of this article can be found at:
DOI: 10.1016/j.jfms.2009.03.003
2009 11: 349Journal of Feline Medicine and SurgeryJacques Penderis
The Wobbly Cat : Diagnostic and Therapeutic Approach to Generalised Ataxia
technique does not amount to an endorsement of its value or quality, or the claims made by its manufacturer.those of the authors and the inclusion in this publication of material relating to a particular product, method orof animals and interpretation of published materials lies with the veterinary practitioner. The opinions expressed arefrom actions or decisions based on information contained in this publication; ultimate responsibility for the treatment
arisingcountry. The authors, editors, owners and publishers do not accept any responsibility for any loss or damageadvertising material, it is the responsibility of the reader to check that the product is authorised for use in their ownbear this in mind and be aware of the prescribing laws pertaining to their own country. Likewise, in relation toFurthermore, drugs may be mentioned that are licensed for human use, and not for veterinary use. Readers need toformulations that are not available or licensed in the individual reader's own country.The Journal of Feline Medicine and Surgery is an international journal and authors may discuss products and
Disclaimer
Published by:
International Society of Feline Medicine
American Association of Feline Practitioners
and
http://www.sagepublications.com
can be found at:Journal of Feline Medicine and SurgeryAdditional services and information for
http://jfm.sagepub.com/cgi/alertsEmail Alerts:
http://jfm.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- May 1, 2009Version of Record>>
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/content/11/5/349http://jfm.sagepub.com/content/11/5/349http://www.isfm.net/http://www.catvets.com/http://www.sagepublications.com/http://www.sagepublications.com/http://jfm.sagepub.com/cgi/alertshttp://jfm.sagepub.com/cgi/alertshttp://jfm.sagepub.com/subscriptionshttp://jfm.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsPermissions.navhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://jfm.sagepub.com/content/11/5/349.full.pdfhttp://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://jfm.sagepub.com/content/11/5/349.full.pdfhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://jfm.sagepub.com/subscriptionshttp://jfm.sagepub.com/cgi/alertshttp://www.sagepublications.com/http://www.catvets.com/http://www.isfm.net/http://jfm.sagepub.com/content/11/5/349http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
2/12
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
3/12
ling the position of the head, trunkand eyeballs. The clinical signs associ-ated with acute, unilateral vestibulardysfunction are asymmetrical andmay include ipsilateral head tilt (Fig2), falling, rolling and vomiting, aswell as nystagmus in both eyes andventrolateral strabismus of the ipsilat-eral eye. Motor strength is maintainedin vestibular ataxia.
Sensory (spinal or general
proprioceptive) ataxiaThe term sensory ataxia is used toindicate the ataxia seen followingdamage to the ascending sensorytracts (most commonly general pro-prioceptive tracts) in the spinal cord.In contrast to cerebellar and vestibularataxia, sensory ataxia is usually associ-ated with concurrent motor involve-ment due to damage to adjacent motor
350 JFMS CLINICAL PRACTICE
R E V I E W /The wobbly cat
tracts within the spinal cord. Lesionsin sensory ataxia are usually confinedto the upper cervical spinal cord(spinal cord segments C1C5), withaffected cats presenting with ataxia,but preservation of the segmentalspinal reflexes, in all four limbs.Lesions further caudal may just affectthe pelvic limbs; alternatively motordeficits, and not ataxia, will tend todominate if the lesion is in the lowercervical region.
Vestibular ataxia canbe further classified asperipheral or central
The neuroanatomical localisation isreasonably well defined in cerebellarand sensory ataxia. However, investibular ataxia, the lesions may besituated either within the peripheralvestibular structures (peripheral
vestibular syndrome) including the innerear (semicircular canals) and vestibulo-cochlear nerve or, less commonly, within the
brain (central vestibular syndrome); thevestibular nuclei of the brainstem are the mostcommon location for central vestibular dis-ease, but other localisations include parts ofthe cerebellum or the thalamus.
Both peripheral and central vestibular syn-drome may present with additional evidenceof deafness, facial nerve paralysis and, in somecases, even sympathetic dysfunction (Fig 3)(Table 2). However, certain deficits are onlyseen in either peripheral or central vestibulardisease and therefore allow differentiationbetween these two sites (Table 3) (Fig 4).
Cerebellar ataxia Vestibular ataxia Sensory (spinal or generalproprioceptive) ataxia
Head movement and position Fine tremor at rest. Intentiontremor with directed movements
Head tilt, usually towards lesion.No head tremor
Normal
Eyeball movementand position
Fine ocular tremor(visible on retinal examination)*
Spontaneous nystagmus andstrabismus*
Normal
Gait Hypermetric. No concurrentmotor weakness
Falling to affected side.Ipsilateral circling or rolling.No concurrent motor weakness
Concurrent motor weakness.Decreased limb proprioception
Posture whenstanding stationary
Abnormal wide-based, swayingand staggering
Relatively normal. Leaning toaffected side
Relatively normal
Other signs Menace response deficits andvestibular signs may be present
Cranial nerve deficits, Hornerssyndrome or ear disease may bepresent. Vomiting may be seenduring actue phase
Cervical pain or deformity may bepresent. Spinal reflexes may benormal to increased
*See box on page 352
Diagnostic approach to the cat with generalised ataxiaTABLE 1
Assessment of patients with subtle ataxia
FIG 2 Domestic shorthair cat with a left head tiltdue to left vestibular syndrome. The involvement ofthe head in cats with generalised ataxia is a usefulmeans of differentiating between the three differentneuroanatomical forms. In sensory ataxia, the headposition is normal; in cerebellar ataxia there isfrequently a fine head tremor or an intentiontremor; in vestibular ataxia there is often a head tiltthat is usually towards the side of the lesion
Maintaining balance when standing in the stationary position requires
proprioceptive, vestibular and visual inputs.
Cats with cerebellar lesions The affected animal is usually unable to
maintain normal balance when standing in the stationary position. It
adopts a wide-based stance and frequently demonstrates a truncal sway
or even stumbling.
Cats with vestibular or sensory lesions The affected animal only requires
two of the three inputs (proprioceptive, vestibular or visual) in order to
maintain balance when standing in the stationary position. Blindfolding
these patients removes the visual input and, if either vestibular or sensory
inputs are affected, then the animals ataxia will worsen and as a result it
will sway or lose its balance.1
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
4/12
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
5/12
8/12/2019 Ataxia Em Gatos
6/12
REV IEW/The wobbly cat
the product normally degraded by thatenzyme starts to accumulate. This accumula-
tion then begins to interfere with cell function-ing. While lysosomes are present in virtuallyevery cell in the body, neurological dysfunc-tion usually predominates. The clinical pres-entation tends to be very specific to theparticular lysosomal storage disease, butthe most common presentation is cerebellarataxia.
Lysosomal storage diseases are uncommon.Affected cats are often normal at birth and
usually present at an early age, demon-strating gradual progression of clinicalsigns. This progression is often the mostuseful way to distinguish these disor-
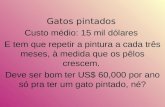
ders from cerebellar hypoplasia, whichis the most common cause of cerebellarataxia in young kittens. There may beadditional clinical signs, or the presen-tation may not be that of cerebellarataxia, depending on the lysosomalstorage disease. Retarded growth, fore-brain dysfunction (including alteredbehaviour and seizures), ocular pathol-ogy (including corneal opacification[Fig 7], cataract and retinal changes),and skeletal and connective tissuechanges (particularly in mucopolysac-
JFMS CLINICAL PRACTICE 353
neurological deficits in cats.4 This is seen lesscommonly in cats than in dogs, with most of
the feline cases reported in the literaturehaving been treated with very high doses ofmetronidazole. The dominant clinical signsare those of central vestibular dysfunction,but may include generalised ataxia, tremors,depression and even seizures. Once clinicalsigns develop discontinuation of metronida-zole is important as continued use may resultin irreversible clinical signs and death.Cessation of therapy in the early stages willusually result in complete and rapidresolution of the clinical signs. Indogs, the use of diazepam will signif-icantly reduce the recovery time, but
this has not been evaluated in cats.
Lysosomal storage diseases
Lysosomal storage diseases representinborn disorders of metabolismresulting from an enzyme deficiencyin the lysosomes, which are thesmall, membrane-bound intracellularorganelles responsible for degrada-tion of cellular and extracellularmaterials. The deficiency or loss offunction is specific to a particularenzyme, with the consequence that
Cerebellar ataxia Peripheral vestibular ataxia Central vestibular ataxia Sensory (spinal or generalproprioceptive) ataxia
Vascular Cerebellar cerebrovascularaccident
Cerebrovascular accidentCerebral ischaemic necrosis
HaemorrhageFibrocartilaginous embolism
Infectious FIP
FSEFungal diseasesParasitic encephalomyelitisToxoplasmosis
Otitis media/interna
Inflammatory polyps
FIP
Fungal diseasesParasitic encephalomyelitisToxoplasmosis
FIP
Fungal diseasesParasitic encephalomyelitisToxoplasmosisEpidural abscess
Idiopathic Idiopathic vestibular syndrome
Toxic Metronidazole Aminoglycoside antibiotics(particularly streptomycin)
Metronidazole
Traumatic Trauma Trauma Trauma Trauma
Anomalous Cerebellar hypoplasia (felinepanleukopenia virus)Intracranial intra-arachnoidcysts
Congenital vestibular syndrome Intracranial intra-arachnoidcysts
Spinal intra-arachnoid cystsCongenital spinal anomaliesFeline Chiari malformation
Neoplastic Brain tumours Tumours invading the inner earand vestibulocochlear nerve(CN VIII)
Brain tumours Spinal cord tumoursVertebral tumours
Nutritional Thiamine deficiency Hypervitaminosis A
Degenerative Lysosomal storage diseasesCerebellar abiotrophy
Intervertebral disc disease
FIP = feline infectious peritonitis, FSE = feline spongiform encephalopathy
Differential diagnoses for the main forms of ataxiaTABLE 4
FIG 7 Corneal opacification in a cat withmucopolysaccharidosis, a lysosomal storage disease
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
7/12
R E V I E W /The wobbly cat
In affected litters, a variable number of
kittens may be involved, with a varying spec-trum of severity between kittens. Clinicalsigns first become apparent when the kittenbegins to walk at around 23 weeks of age,with affected kittens demonstrating evidenceof diffuse cerebellar involvement. The clinicalsigns are non-progressive; in fact, some clini-cal improvement may become apparent insome kittens, presumably because of compen-sation through other senses such as generalproprioception and vision.
The finding of diffuse cerebellar signs, withthe absence of progression and lack of involve-ment of other areas of the CNS, is usuallysufficient to make a diagnosis of cerebellarhypoplasia. Establishing a definitive ante-mortem diagnosis is difficult and usually restson demonstrating a small cerebellum followingadvanced imaging (usually MRI). Whilethere is no treatment for cerebellar hypoplasia,less severely affected kittens make acceptablepets, particularly if substantial compensationoccurs.
Intracranial intra-arachnoid cystsQuadrigeminal cysts are intracranial cysticaccumulations of CSF within the arachnoid
mater at the level of the quadrigeminal cistern.Controversy surrounds the clinical significanceof these cysts, which are rare in cats, with manybeing detected as apparently incidental find-ings. Neurological deficits may become evidentif gradual expansion of a quadrigeminal cystresults in increased intracranial pressure,compression of adjacent neural structures orobstruction of CSF outflow pathways (Fig 10).8
charidosis) may also be evident (Fig 8).
A strong presumptive diagnosis can often bemade on the basis of the cats age, clinical pres-entation and progression of signs. This clinicalsuspicion can be strengthened by demonstrat-ing the accumulation of storage products orvacuoles in leukocytes or tissue biopsy samples(usually liver, spleen or lymph node).Confirmation of the diagnosis relies on lysoso-mal enzyme analysis in cases where the enzymedefect is known, and genetic testing where the
genetic defect has beenidentified.5 In somedisorders the storageproduct may bedemonstrated on urineanalysis or muscle andnerve biopsy.
Regardless of thediagnosis, the progno-sis is poor.
Cerebellar hypoplasia
Cerebellar hypoplasia (caused by feline pan-leukopenia virus) has historically been recog-nised in kittens, but it was only in the 1960sthat experimental and spontaneous in utero
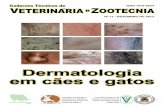
infection of pregnant cats with the panleukope-nia virus was demonstrated to cause cerebellarhypoplasia in the progeny.6 Since this timemost cases of cerebellar hypoplasia in kittenshave been attributed to in utero panleukopeniavirus infection and in dogs to parvovirus.7 Thepanleukopenia virus has cytopathic effects onrapidly dividing cells, particularly the granulecell layer of the cerebellum. As a result, thecerebellum of affected kittens is grosslyhypoplastic (Fig 9), with some having concur-rent hydrocephalus or hydranencephaly.
354 JFMS CLINICAL PRACTICE
FIG 8 Cervical rigidity withdecreased range of movementdue to fusion of the cervicalvertebrae in a cat withmucopolysaccharidosis.
An important differentialdiagnosis for cervical fusiondue to proliferative bonylesions is hypervitaminosis A;in both diseases the bony
lesions may result in spinalcord compression andgeneralised ataxia
FIG 9 Cerebellar hypoplasia is common in young kittens and occasionally seen in youngpuppies. The cerebellum is grossly smaller (right) than in the normal kitten (left). Clinicallythis decrease in cerebellar size can be identified on MRI scans as a decreased size of thecerebellum or increased CSF dissecting between the folia of the cerebellum
FIG 10 Typical appearance of a quadrigeminal cyst ona parasagittal T2-weighted MRI scan. The majority ofquadrigeminal cysts are incidental findings; however, if acyst becomes very large then it may result in compressionof adjacent neurological tissues, as in this case
In litters with cerebellar hypoplasia, a variable number of kittens may be affected,
with a varying spectrum of severity between kittens. Cerebellar hypoplasia
is characterised by diffuse cerebellar signs with an absence of progression.
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
8/12
REV IEW/The wobbly cat
JFMS CLINICAL PRACTICE 355
Otitis media/internaThis common cause of vestibularsigns is usually associated with exten-sion of otitis externa into the middleand inner ear, but may arise in theabsence of external ear canal inflam-mation. Foreign bodies in the externalear canals (eg, grass awns) may pene-
trate the tympanic membrane orcause a chronic otitis externa withrupture of the tympanic membrane.In the absence of otitis externa, twoother routes of infection include retro-grade spread via the Eustachian tubesand haematogenous spread. The mostcommon infectious agents arebacteria, including Staphylococcus ,Streptococcus , Proteus, Pseudomonasspecies, Enterococcus species andEscherichia coli. If otitis media/internais suspected, but bacterial cultureresults are not available, then thechoice of antibiotic is usually basedon sensitivity to the above bacteria. Ear mites(Otodectes cynotis) in cats may also result inrupture of the tympanic membrane and asecondary otitis media/interna.
The clinical signs associated with otitismedia/interna usually reflect an acute onset
of peripheral vestibular syndrome,and a partial recovery may becomeapparent as the animal compensatesfor the vestibular deficits over thenext day or two. In some cases theremay be evidence of intracranialdisease if the otitis media erodesthrough the calvarium (Fig 11), but
these cats will also have obviousevidence of middle ear disease.In contrast to idiopathic vestibular
syndrome (see later) there are usuallysecondary clinical signs related to theear infection. These may include: Discharge from the external earcanal, with head shaking, scratchingor rubbing of the ears and frequentyawning; Abnormalities on auroscopicexamination of the tympanic bulla; Pain on opening the mouth orpalpation of the structures adjacentto the ear;
Damage to adjacent nervous systemstructures, in particular the facial nerve andsympathetic supply to the head (Hornerssyndrome). Less commonly facial nervedysfunction may also include damage to theparasympathetic supply to the lacrimalglands, resulting in a dry eye and nose; Hemifacial spasm where there is earlyirritation of the facial nerve, although this isless common.
Diagnosis of otitis media/interna is basedon findings of peripheral vestibular syndrome
and typical clinical signs of ear disease,together with auroscopic examination of thetympanic membrane, radiography oradvanced imaging of the head (Figs 12 and 13)and, possibly, surgical exploration.9 If there is
FIG 11 Transverse T1-weighted MRI scan following IVadministration of gadolinium contrast medium. Otitismedia/interna (solid arrow) is usually associated withperipheral vestibular syndrome, but (particularly incats) it is not unusual for infection to erode throughinto the calvarium and result in secondary meningitis(hyperintensity of the meninges and falx cerebri; openarrows). The investigation of cats with centralvestibular disease (25% of cases of which may haveconcurrent seizures) should therefore still include anevaluation of the middle ear
FIG 12 MRI images from the cat pictured in Fig 3 with otitis media, showing inflammationaffecting the soft tissues adjacent to the bulla. (a) Transverse T2-weighted scan; (b) T1-weighted pre-contrast scan; (c) T1-weighted post-contrast scan; and (d) subtraction scan(ie, image [c] subtracted from image [b] in order to demonstrate the contrast enhancement).The air cavity within the bulla is obliterated (arrows in [a] and [b]) and there is marked contrastenhancement adjacent to the bulla (arrows in [c] and [d])
FIG 13 Dorsal T2-weighted MRI scan from the cat picturedin Fig 3, demonstrating obliteration of the air cavity within thebulla (closed arrow) by a hyperintense signal (open arrow)
a b
c d
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
9/12
8/12/2019 Ataxia Em Gatos
10/12
8/12/2019 Ataxia Em Gatos
11/12
R E V I E W /The wobbly cat
358 JFMS CLINICAL PRACTICE
Intervertebral disc diseaseWhile intervertebral disc disease is an impor-tant canine neurological problem, accountingfor over 2% of all diseases diagnosed in thedog, it is uncommon in cats.20 In most catsintervertebral disc disease is noted as an inci-dental finding (Fig 17), but in occasional casesit may be clinically relevant. In cats that do
present with suspected intervertebral disc dis-ease, there are clinical signs of pain or varyingdegrees of spinal cord dysfunction.
Intervertebral disc disease in the cat is usu-ally Hansen type I, where herniation of thenucleus pulposus occurs through the annularfibres of the disc into the spinal canal (versustype II, where annular protrusion into thespinal canal is caused by shifting of the nucle-us pulposus material).
Cerebral ischaemic necrosis
A syndrome of cerebral infarction has beenrecognised in cats so-called cerebralischaemic necrosis or feline ischaemicencephalopathy. The lesion usually affects thecerebral cortex, but the brainstem is affectedin some cats and multiple regions in othercats. The underlying cause of the vascularlesion is usually not identified, although it hasbeen demonstrated to be associated withcuterebriasis in some cases.21 The diseaseaffects adult cats of both sexes and a numberof breeds. The clinical signs are peracute inonset, non-progressive and usually resolvecompletely over a period of several weeks.Computed tomography or MRI support the
diagnosis and CSF analysis usually demon-strates mild elevation of protein, withoutinflammation. Treatment is largely support-ive, but corticosteroids may helpto reduce brain oedema and anti-convulsants are indicated in catswith seizures.
Thiamine deficiency
Thiamine (as thiamine pyrophos-phate) is important in carbohy-drate and amino acid metabolism.Thiamine deficiency causes a pro-gressive encephalopathy in cats,
other animals and in humanpatients, with species-specificselective vulnerability withinspecific brain regions.22
Thiamine deficiency in cats canbe due to a variety of causes,including a diet high in fish, excessive heatingof food and excessive levels of sulphite preser-vatives in the food. Affected cats frequentlydemonstrate a period of anorexia precedingthe onset of neurological signs. The neuro-logical deficits are usually multifocal, butevidence of vestibular dysfunction predomi-
FIG 17 Intervertebral disc disease is uncommon in the cat. In most cases it is identified asan incidental finding, as in this case with calcification of the nucleus pulposus of the discsbetween the T11T12 and T12T13 vertebrae
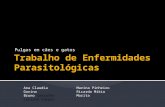
FIG 18 Transverse T2-weighted MRI scandemonstrating bilaterallysymmetrical hyperintensity ofthe lateral geniculate nuclei(arrow) in a cat with thiaminedeficiency. Hyperintensity ina variety of brain nucleisupports the clinicalsuspicion of thiaminedeficiency in affected animals
nates. Typically, ataxia, intermittent verticalnystagmus, bilateral absent menace respons-es, anisocoria and episodes of severe vestibu-lar disturbance are seen. There may also beevidence of cervical ventroflexion, muscleweakness and fixed, dilated pupils. The con-dition can progress to seizures, coma anddeath.
The preferred diagnostic method is meas-urement of transketolase activity in fresh ery-throcytes. If this is not possible the metaboliceffects of thiamine deficiency can be demon-
strated by urinary organic acid analysis.Dietary thiamine can be determined byhigh performance liquid chromatography.
Magnetic resonance imaging canbe used to confirm a suspectedcase; thiamine deficiency isdemonstrated by a characteristicpattern of bilaterally symmetricalhyperintensity on T2-weightedand FLAIR images within avariety of brain nuclei andregions, including the lateralgeniculate nuclei, caudal colliculi,periaqueductal grey matter,
medial vestibular nuclei, cerebel-lar nodulus and facial nuclei(Fig 18).23
Treatment should be started assoon as possible with intravenousfluid therapy, nasogastric tube
feeding and intramuscular thiamine injections(Vitamin B1 Injection; Bimeda VeterinaryPharmaceuticals) at 25 mg once daily.Thiamine therapy should continue until thecat demonstrates improvement or a satisfacto-ry oral intake of thiamine; generally around5 days should suffice.
at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/8/12/2019 Ataxia Em Gatos
12/12
Acknowledgements
The author is grateful to Mr Richard Irvine, VeterinaryPathological Sciences, University of Glasgow, for the grosspathological image in Fig 6, Dr Hal Thompson, VeterinaryPathological Sciences, University of Glasgow, for the grosspathological image in Fig 9, and to Mr Ronny Barron,Companion Animal Diagnostics, University of Glasgow, forthe image of lymphoma cells within the CSF (Fig 15).
References
1 Khasnis A, Gokula R. Rombergs test. J Postgrad Med 2003; 49:
16972.
2 Bradshaw JM, Pearson GR, Gruffydd-Jones TJ.
A retrospective study of 286 cases of neurological disorders of thecat.J Comp Pathol 2004; 131: 11220.
3 Boettcher IC, Steinberg T, Matiasek K, Greene CE, Hartmann K,
Fischer A. Use of anti-coronavirus antibody testing of cere-
brospinal fluid for diagnosis of feline infectious peritonitis involv-
ing the central nervous system in cats. J Am Vet Med Assoc 2007;
230: 199205.
4 Caylor KB, Cassimatis MK. Metronidazole neurotoxicosis in two
cats.J Am Anim Hosp Assoc 2001; 37: 25862.
5 Skelly BJ, Franklin RJ. Recognition and diagnosis of lysosomal
storage diseases in the cat and dog. J Vet Intern Med 2002; 16:
13341.
6 Kilham L, Margolis G, Colby ED. Congenital infections of cats
and ferrets by feline panleukopenia virus manifested by cerebel-
lar hypoplasia. Lab Invest 1967; 17: 46580.
7 Schatzberg SJ, Haley NJ, Barr SC, et al. Polymerase chain reaction
(PCR) amplification of parvoviral DNA from the brains of dogs and
cats with cerebellar hypoplasia.J Vet Intern Med 2003; 17: 53844.
8 Lowrie M, Wessmann A, Gunn-Moore D, Penderis J.
Quadrigeminal cyst management by cystoperitoneal shunt
in a 4-year-old Persian cat. J Feline Med Surg.
doi:10.1016/j.jfms.2009.01.007
9 Sturges BK, Dickinson PJ, Kortz GD, et al. Clinical signs, magnet-
ic resonance imaging features, and outcome after surgical and
JFMS CLINICAL PRACTICE 359
REV IEW/The wobbly cat
Generalised ataxia may be due to disease affecting the cerebellum, vestibular system or cervical spinal cord,
and each of these regions has characteristic clinical signs.
Cerebellar hypoplasia is the most important cause of generalised ataxia in young kittens, and is characterised
by diffuse, non-progressive cerebellar signs.
Feline infectious peritonitis is an important cause of generalised ataxia in juvenile and older cats; it usuallyaffects the cerebellum, but may also affect the central vestibular system and spinal cord.
Otitis media in cats may erode through into the calvarium, resulting in signs of brain disease
(including seizures). Evaluation of the ear canals is therefore important, even if cats present with
evidence of central vestibular disease.
Thiamine deficiency should be considered in any cat with a previous history of anorexia that
subsequently develops evidence of progressive central vestibular disease.
KEYPOINTS
medical treatment of otogenic intracranial infection in 11 cats and
4 dogs.J Vet Intern Med 2006; 20: 64856.
10 Muilenburg RK, Fry TR. Feline nasopharyngeal polyps. Vet Clin
North Am Small Anim Pract 2002; 32: 83949.
11 Burke EE, Moise NS, de Lahunta A, Erb HN. Review of idiopath-
ic feline vestibular syndrome in 75 cats.J Am Vet Med Assoc 1985;
187: 94143.
12 Reder MS, Mathog RH, Capps MJ. Comparison of caloric and
sinusoidal tests in the vestibulotoxic cat. Laryngoscope 1977; 87:
200815.
13 James CC, Lassman LP, Tomlinson BE. Congenital anomalies of
the lower spine and spinal cord in Manx cats. J Pathol 1969; 97:
26976.
14 Bichsel P, Vandevelde M, Lang J. Spinal cord infarction following
fibrocartilaginous embolism in the dog and cat. Schweiz Arch
Tierheilkd 1984; 126: 38797.15 Mikszewski JS, Van Winkle TJ, Troxel MT. Fibrocartilaginous
embolic myelopathy in five cats.J Am Anim Hosp Assoc 2006; 42:
22633.
16 Marioni-Henry K, Van Winkle TJ, Smith SH, Vite CH. Tumors
affecting the spinal cord of cats: 85 cases (19802005). J Am Vet
Med Assoc 2008; 232: 23743.
17 Lane SB, Kornegay JN, Duncan JR, Oliver JE. Feline spinal lym-
phosarcoma: a retrospective evaluation of 23 cats.J Vet Intern Med
1994; 8: 99104.
18 Seawright AA, English PB. Hypervitaminosis A and deforming
cervical spondylosis of the cat. J Comp Pathol 1967; 77: 2939.
19 Polizopoulou ZS, Kazakos G, Patsikas MN, Roubies N.
Hypervitaminosis A in the cat: a case report and review of the
literature.J Feline Med Surg 2005; 7: 36368.
20 Knipe MF, Vernau KM, Hornof WJ, LeCouteur RA. Intervertebral
disc extrusion in six cats.J Feline Med Surg 2001; 3: 16168.
21 Williams KJ, Summers BA, de Lahunta A. Cerebrospinal cutere-
briasis in cats and its association with feline ischemic
encephalopathy. Vet Pathol 1998; 35: 33043.
22 Jubb KV, Saunders LZ, Coates HV. Thiamine deficiency
encephalopathy in cats.J Comp Pathol 1956; 66: 21727.
23 Penderis J, McConnell FJ, Calvin J. Magnetic resonance imaging
features of thiamine deficiency in a cat. Vet Rec 2007; 160: 27072.
Available online at www.sciencedirect.com at UNIV REGIONAL DE BLUMENAU on March 23, 2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/