







Línguas
Páginas
Legal

Six Month Results of the Global BIOLUX P-III All-Comers Registry using Drug Coated Balloon in Infra-Inguinal Artery Disease
Dr. Shaiful Azmi Yahaya, FNHAM, FAPSIC Institut Jantung Negara, Kuala Lumpur, Malaysia
CCI on behalf of the BIOLUX P-III Investigators
Disclosure
• Speaker name: Dr. Shaiful Azmi Yahaya
I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
X I do not have any potential conflict of interest

Passeo-18 Balloon
Catheter
Balloon Platform
Improves ease of handling
Protects the user and balloon from contact and damage
SafeGuard Insertion Aid
Drug: Paclitaxel
Excipient: Butyryl-Trihexyl Citrate (BTHC)
Coating
Passeo-18 Lux combines proven technologies for treating lower limb arteries

Paclitaxel blocks the cell cycle directly
Paclitaxel inhibits the cell cycle directly vs. Limus drugs which act indirectly DCB‘s aim for a high-dose effect of Paclitaxel, causing cell‘s mitotic arrest A low-dose effect is expected to sustain antiproliferation long term
Mode of action for Paclitaxel and Limus drugs
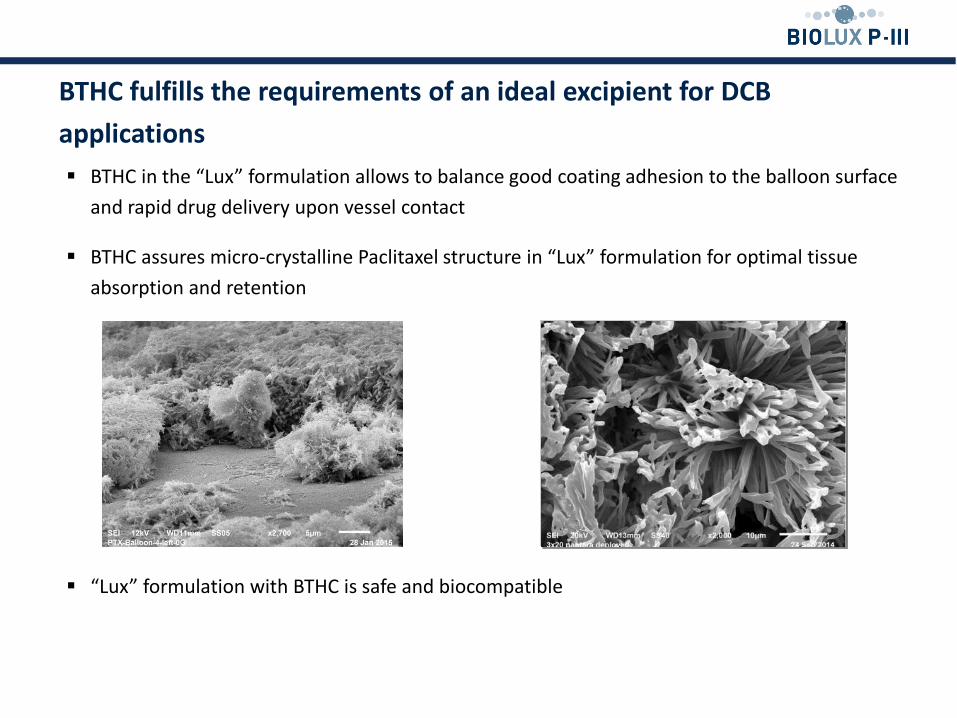
BTHC in the “Lux” formulation allows to balance good coating adhesion to the balloon surface
and rapid drug delivery upon vessel contact
BTHC assures micro-crystalline Paclitaxel structure in “Lux” formulation for optimal tissue
absorption and retention
“Lux” formulation with BTHC is safe and biocompatible
BTHC fulfills the requirements of an ideal excipient for DCB
applications

6
GAP 2015
Passeo-18 Lux Clinical Trial Program
Study Device(s) Indication Design Primary
Endpoint PI(s)
Passeo-18 Lux
vs. Passeo-18 SFA
EU Multicenter FIM RCT
(60 pts/5 sites) LLL @6m D. Scheinert
Passeo-18 Lux
vs. Passeo-18 BTK
EU Multicenter FIM RCT
(72 pts/6 sites)
MAE@1m
PP@6m T. Zeller
Passeo-18 Lux
Infrainguinal
Arteries
Global Multicenter All-
comers
Registry
(min. 700 pts/55 sites)
MAE@6m
FTLR@12m G. Tepe
Passeo-18 Lux
+ Pulsar-18 SFA
EU Multicenter Single-arm
trial (120 pts/5 sites) PP@12m M. Bosiers
Passeo-18 Lux
vs. PTA
AV Fistula
Access
Canadian Multicenter RCT
(120 pts/4 sites) LLL@6m E. Terasse
Passeo-18 Lux
+ Pulsar-18 SFA
Australian Single-arm trial
(100 pts)
PP@12m
PP@24m P. Mwipatayi
Passeo-18 Lux In-stent
restenosis
Australian Retrospective
registries
(35* pts / 29° pts)
PP, FTLR, MAE
@6m
P. Myers*
D. Robertson°
*Investigator-Initiated Trials
*
*
*
*

7
GAP 2015
BIOLUX P-I 6 month Late Lumen Loss Comparison of Peripheral DEB RCTs
References: BIOLUX P-I. Scheinert et al. Presented at EuroPCR 2012 THUNDER Tepe et al: N Engl J Med. 2008 Feb 14;358(7):689-99. FEMPAC Werk et al: Circulation. 2008;118:1358-1365. PACIFIER Werk et al: Circ Cardiovasc Interv. 2012 Dec;5(6):831-40 LEVANT-I: Scheinert et al.: JACC: Cardiovasc Interv. 2014; 7(1): 10-19.

8
GAP 2015
Death Major
Amputation TLR TVR
TL
Thrombosis
DCB (%) 0.0% 0.0% 0.0% 0.0% 0.0%
POBA (%)
[CI] 0.0%
2.8%
[0.4-18.1]
5.6%
[1.4-20.7]
5.6%
[1.4-20.7] 0.0%
p-value - 1.000 0.493 0.493 -
p* < 0.05 significant
BIOLUX P-II: Brodmann M Presented at LINC 2014
Major Adverse Events at 30 days Adjudicated by an Independent Clinical Events Committee
Time to Event (days)
POBA 8.3% [2.8 – 23.7]
DCB 0.0% [0.0 – 0.0] 0%
10%
20%
30%
40%
50%
0 30
MAE (%)
p-value : 0.239 (Fisher‘s exact)
p-value : 0.239 (Fisher‘s Exact)
9
GAP 2015
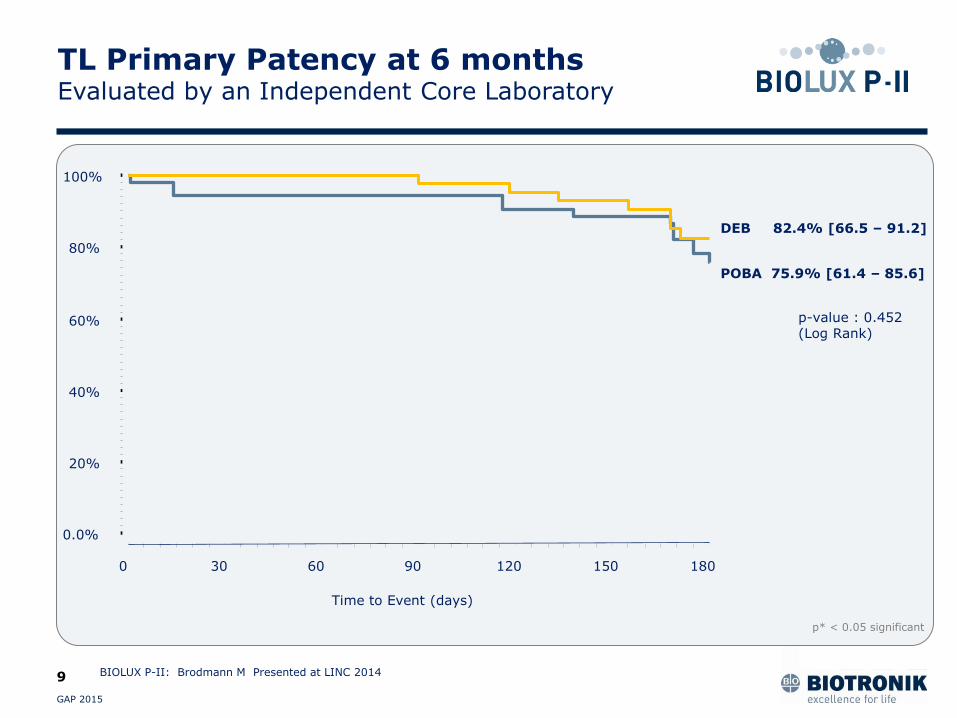
BIOLUX P-II: Brodmann M Presented at LINC 2014
0.0%
20%
40%
60%
80%
100%
Time to Event (days)
0 30 60 90 120 150 180
POBA 75.9% [61.4 – 85.6]
DEB 82.4% [66.5 – 91.2]
p-value : 0.452 (Log Rank)
TL Primary Patency at 6 months Evaluated by an Independent Core Laboratory
p* < 0.05 significant
Six Month Results of the Global BIOLUX P-III All-Comers Registry using Drug Coated Balloon in Infra-Inguinal Artery Disease

Participating Sites 204 Subjects Reached 6 Month FUP
# Subject enrolled #Subjects enrolled up to
25th Jan 2016
Pr G. Tepe (CCI) RoMed Klinikum Rosenheim Germany 3 36
Pr M. Brodmann Medical University Graz Austria 72 120
Pr T. Zeller Universitäts-Herzzentrum Freiburg - Bad Krozingen Germany 28 84
Dr J. K. Christensen Kolding Hospital Denmark 15 28
Dr L. Spak VUSCH East Slovak Cardiology Institute Slovakia 12 42
Pr C. Binkert Kantonspital Winterthur Switzerland 12 19
Dr H. Schröder Jüdischen Krankenhaus Berlin Germany 11 20
Pr G. Nano, Policlinico San Donato Italy 8 15
Dr M. Araujo Hospital Universitaro Severo Ochoa Spain 7 16
Dr L. Yo Catharina Ziekenhuis Eindhoven Hospital Netherlands 6 13
Dr J. Dahm Herz-und Gefässzentrum Göttingen Germany 5 18
Pr F. Hammer Cliniques Universitaires Saint-Luc Belgium 5 6
Dr S. Houthoofd UZ Leuven Belgium 5 10
Dr M. Lichtenberg Klinikum Arnsberg Germany 3 10
Dr S. Kum Changi General Hospital Singapore 2 4
Pr J.L. Magne Centre Hospitalier Universitaire de Grenoble France 2 7
Dr J.M. Romero Hospital Universitari Santa Creu i Sant Pau Spain 3 8
Dr D. Kretzschmar Universitätsklinikum Jena Germany 2 6
Dr E. Alejandre-Lafont Universitätsklinikum Giessen und Marburg Germany 2 14
Dr D. Henroteaux CHR de la Citadelle de Liège Belgium 1 13
Later initiated sites 0 171
204 660
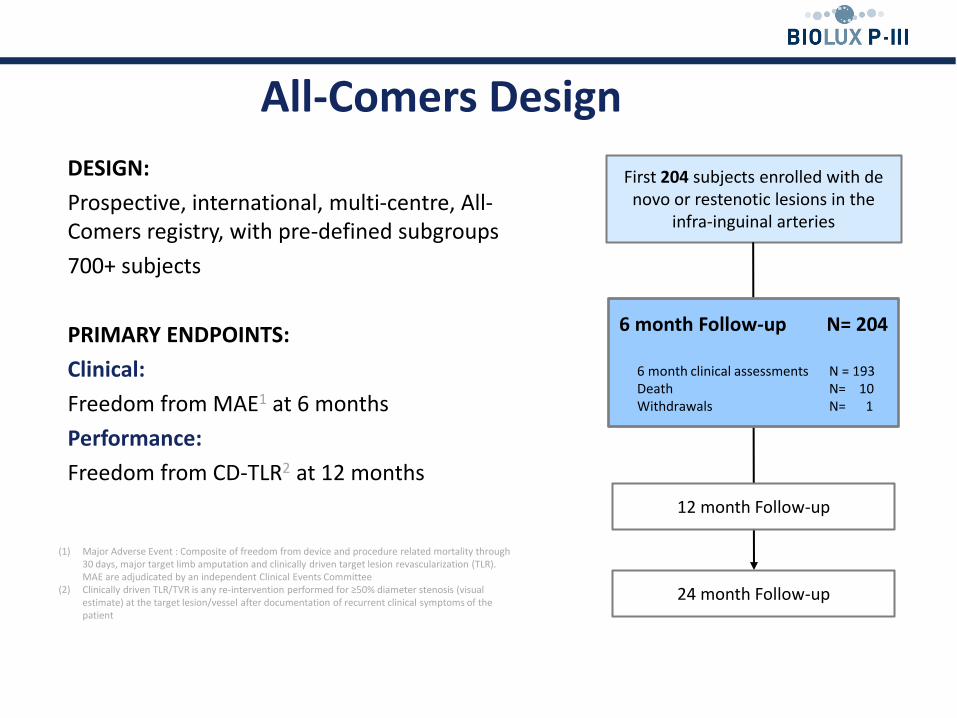
DESIGN:
Prospective, international, multi-centre, All-Comers registry, with pre-defined subgroups
700+ subjects
PRIMARY ENDPOINTS:
Clinical:
Freedom from MAE1 at 6 months
Performance:
Freedom from CD-TLR2 at 12 months
First 204 subjects enrolled with de novo or restenotic lesions in the
infra-inguinal arteries
24 month Follow-up
12 month Follow-up
6 month Follow-up N= 204
6 month clinical assessments N = 193 Death N= 10 Withdrawals N= 1
All-Comers Design
(1) Major Adverse Event : Composite of freedom from device and procedure related mortality through 30 days, major target limb amputation and clinically driven target lesion revascularization (TLR). MAE are adjudicated by an independent Clinical Events Committee
(2) Clinically driven TLR/TVR is any re-intervention performed for ≥50% diameter stenosis (visual estimate) at the target lesion/vessel after documentation of recurrent clinical symptoms of the patient

Baseline Characteristics
Age, yrs (mean ± SD), [Min; Max] 70.2 ± 10.4 [44.0 ; 94.0]
Male (n, %) 123 (60.3%)
Medical History N= 204 %
Hypertension 176 86.3%
Hyperlipidemia 144 70.6%
Smoking Current Smokers
139 53
68.1% 38.1%
History of PAOD 121 59.3%
Previous PVI /Surgeries 113 55.4%
Diabetes 97 47.5%
Coronary Artery Disease 78 38.2%
Cerebrovascular Disease 50 24.5%
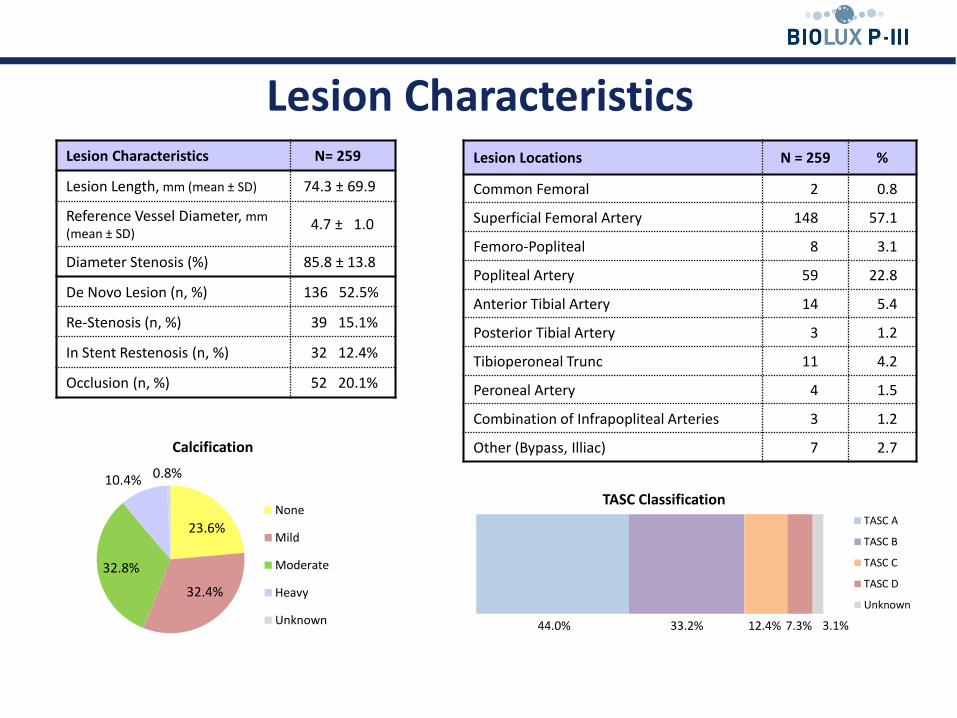
Lesion Characteristics Lesion Characteristics N= 259
Lesion Length, mm (mean ± SD) 74.3 ± 69.9
Reference Vessel Diameter, mm (mean ± SD)
4.7 ± 1.0
Diameter Stenosis (%) 85.8 ± 13.8
De Novo Lesion (n, %) 136 52.5%
Re-Stenosis (n, %) 39 15.1%
In Stent Restenosis (n, %) 32 12.4%
Occlusion (n, %) 52 20.1%
Lesion Locations N = 259 %
Common Femoral 2 0.8
Superficial Femoral Artery 148 57.1
Femoro-Popliteal 8 3.1
Popliteal Artery 59 22.8
Anterior Tibial Artery 14 5.4
Posterior Tibial Artery 3 1.2
Tibioperoneal Trunc 11 4.2
Peroneal Artery 4 1.5
Combination of Infrapopliteal Arteries 3 1.2
Other (Bypass, Illiac) 7 2.7
23.6%
32.4%
32.8%
10.4% 0.8%
Calcification
None
Mild
Moderate
Heavy
Unknown 44.0% 33.2% 12.4% 7.3% 3.1%
TASC Classification TASC A
TASC B
TASC C
TASC D
Unknown
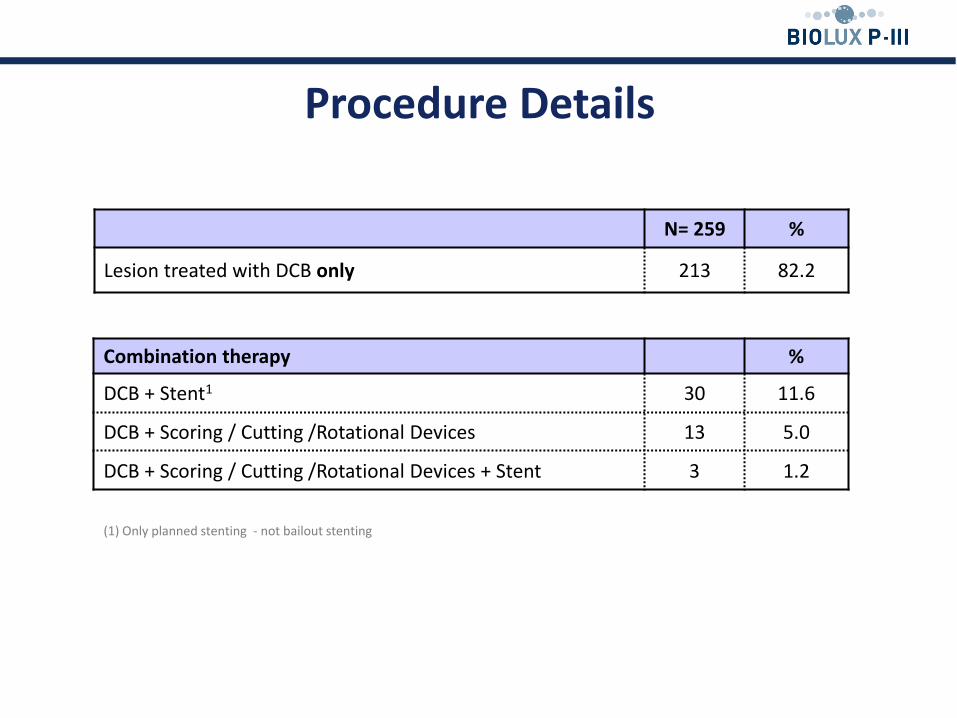
Procedure Details
N= 259 %
Lesion treated with DCB only 213 82.2
(1) Only planned stenting - not bailout stenting
Combination therapy %
DCB + Stent1 30 11.6
DCB + Scoring / Cutting /Rotational Devices 13 5.0
DCB + Scoring / Cutting /Rotational Devices + Stent 3 1.2

Freedom From MAE (adjudicated by an independent CEC)
Free
do
m f
rom
MA
E
Time to events (days)
94.4% SE 0.0163 CI95% [ 90.2, 96.9]
MAE (composite of procedure or device related death within 30 days post index procedure, CD-TLR, Target Limb Major amputation)
11 94.4%
Death 1 99.5%
Clinically Driven Target Lesion Revascularization 8 96.8%
Target Limb Major Amputation 2 99.0%
N= 143
Surv
ival
Estim
ate:
MAE
0.0%
20%
40%
60%
80%
100%
Time to Event (days)
0 30 180

Surv
ival
Estim
ate:
Clin
ical
ly d
riven
TLR
0.0%
20%
40%
60%
80%
100%
Time to Event (days)
0 30 180
Freedom From Clinically Driven Target Lesion Revascularization1
Time to events (days)
Free
do
m f
rom
Clin
ical
ly D
rive
n T
LR
96.8% SE 0.0112 CI95%[ 93.7, 98.4]
N= 186
(1) Any re-intervention performed for ≥ 50% diameter stenosis (visual estimate) at the target lesion after documentation of recurrent clinical symptoms of the patient
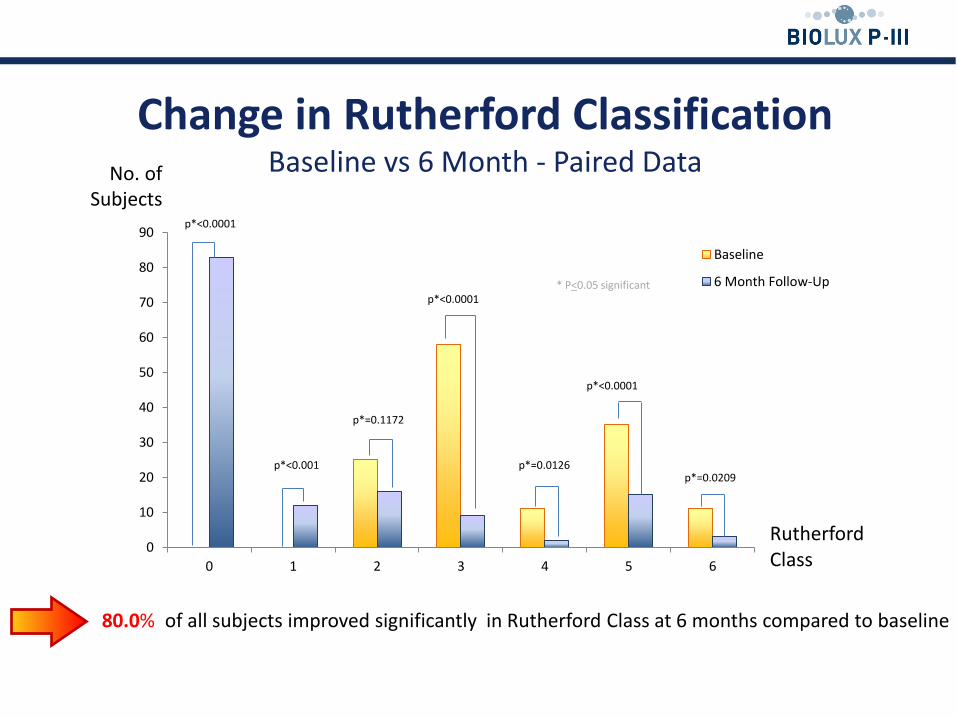
Change in Rutherford Classification Baseline vs 6 Month - Paired Data
0
10
20
30
40
50
60
70
80
90
0 1 2 3 4 5 6
Rutherford Class
Baseline
6 Month Follow-Up
p*<0.0001
p*<0.001
p*=0.1172
p*<0.0001
p*<0.0001
p*=0.0209 p*=0.0126
80.0% of all subjects improved significantly in Rutherford Class at 6 months compared to baseline
* P<0.05 significant
No. of Subjects

0
10
20
30
40
50
60
70
80
90
100
No hurt Hurts little bit Hurts little more Hurts even more Hurts whole lot Hurts worst
Baseline
6 Month Follow-Up
P*=0.1282 P*=0.6015
P* <0.0001
P*<0.0001
P*=0.0325
P*<0.05 significant
P*<0.0001
Change in Pain Scale1
Baseline vs 6 Month - Paired Data
80.4% of all subjects improved significantly in Pain Scale at 6 months compared to baseline
No. of Subjects
(1) Wong-Baker FACES Pain Rating Scale

Conclusion
BIOLUX P-III is a real All-Comers Registry evaluating the performance of DCB in daily practice in respect to patient and lesion characteristics and combination therapy
6 Months results of the first 200 subjects present comparable safety and performance results:
96.8 % Freedom from Clinically Driven Target Lesion Revascularization
80.0 % of subjects improved significantly in Rutherford classification (p<0.001)
80.4% subjects experienced significantly less pain at 6 months compared to baseline (p<0.001)
Further subgroup analysis will reveal even more insight in daily routine practice – specifically DCB in combination therapy

Thank You

Six Month Results of the Global BIOLUX P-III All-Comers Registry using Drug Coated Balloon in Infra-Inguinal Artery Disease
Dr. Shaiful Azmi Yahaya, FNHAM, FAPSIC Institut Jantung Negara, Kuala Lumpur, Malaysia
CCI on behalf of the BIOLUX P-III Investigators
Top Related