Suturando para sucesso cirúrgico.pdf

of 11
Transcript of Suturando para sucesso cirúrgico.pdf
-
7/27/2019 Suturando para sucesso cirrgico.pdf
1/11
Suturing for Surgical Success
Written by Gregori M. Kurtzman, DDS Saturday, 01 October 2005 00:00
Surgery involves the creation of a wound, and proper closure of this wound is usually
necessary to promote optimal healing. Suturing a wound positions and secures the
surgical flaps to promote healing. Surgical sutures should hold the edges of a flap in
apposition until the wound has healed sufficiently to withstand normal functional
stresses and resist reopening.
Table 1. General Guidelines for Suturing.
Sutures are usually first placed distal to the last tooth,
in each interproximal space, with suturing continued in
a mesial direction.
First insert sutures through the more mobile tissue flap.
When space is restricted, use a one-half circle needle.
Only needle holders should be used to grasp suture
needles, and the suture needle should be inserted and
pulled through the issue in line with the curve of the
needle.
Grab the suture needle in the center of the needle,
never at its tip or near where the thread is swage to the
needle.
When suturing multiple tissue levels, the goal is to
suture periosteum to periosteum and gingival tissue togingival tissue. (Note: The connective tissue and
epithelial layers are together being referred to as
gingival tissue.)
The needle should enter tissue at right angles to the
tissue.
Do not place sutures closer than 2 mm to 3 mm from
the flap edges to prevent tearing through the flap
during suturing, or if postoperative swelling occurs.
http://www.dentistrytoday.com/periodontics/359-suturing-for-surgical-successhttp://www.dentistrytoday.com/periodontics/359-suturing-for-surgical-successhttp://www.dentistrytoday.com/periodontics/359-suturing-for-surgical-success -
7/27/2019 Suturando para sucesso cirrgico.pdf
2/11
When suturing, flaps should be approximated without
blanching of the tissue. Pull the suture just tight
enough to secure the flap in place without restricting
the flap's blood supply.
In addition to proper technique, it is critical to select the appropriate type and size(diameter) of suture material to ensure that wound margins are free of tension, allowing
healing by primary intention.1 Accurate apposition of surgical flaps contributes to
patient comfort, hemostasis, reduction of wound size, and prevention of unnecessary
bone resorption. If surgical wound edges are not properly approximated, hemostasis can
be compromised and blood/serum may accumulate under the flap. This could result in a
space between the underlying soft tissue and bone, thus delaying the healing process.2 In
addition, when this occurs, healing will be by secondary intention, which can lead to
irregular soft-tissue contours and the formation of scar tissue (Table 1).
Conventional intraoral surgical treatment concludes with closure of the soft tissue.
Proper suturing precisely positions the mucosal and/or mucoperiosteal flaps as required
by the surgical procedure being performed. Certain periodontal surgical procedures (eg,
excisional new attachment procedure [ENAP] and modified Widman flap procedure)
require the surgical flap margins to be positioned in their original location, whereas
other periodontal procedures may require that the surgical flaps be placed apically,
coronally, or laterally to their original position in order to achieve the surgical
objectives.3
Suturing technique, the type and diameter of suture material (thread), the type of
surgical needle, and the design of the surgical knot are essential factors in achieving
optimal wound healing. Wound closure variables are different when suturing over hardversus soft tissue, or suturing over various types of materials placed into the surgical
site to promote periodontal regeneration (eg, bone graft material or a membrane). The
suture material and needle design will change accordingly.
This article will discuss suturing materials and certain useful suture knot designs, with a
focus on periodontal surgical procedures.
MATERIAL COMPONENTS
Needles
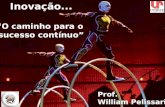
Figure 1. Comparison of a
one-half circle needle (top)
and three-eighths circle needle
-
7/27/2019 Suturando para sucesso cirrgico.pdf
3/11
The surgical needle is composed of the point, the body, and the swaged (press-fit) end.
Classification of suture needles is usually based on their curvature, radius, and shape.
For intraoral use, three-eighths and one-half circle needles are most commonly used3,4
(Figure 1).
When using the three-eighths needle to close tissue in the oral cavity, the clinicianrotates the needle on a central axis to pass it from the buccal surface to the lingual
surface in one motion, whereas the one-half circle needle is traditionally used in more
restricted areas (eg, buccal surface of maxillary molars and facial surface of maxillary
and mandibular incisors). The one-half circle needle is routinely used for periosteal and
mucogingival surgery.1-4
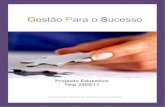
Figure 2. Conventional needle
(left) and reverse-cutting
needle
Suture needles may also be classified as either conventional cutting or reverse cutting.5
In the oral cavity, reverse-cutting sutures should be used to prevent the suture material
from tearing through the papillae or edges of the surgical flap (referred to as "cut out" ).
Conventional su-ture needles are generally associated with cut out because the inside
concave (inner) curvature is sharpened; as the needle is pulled through the tissue, it cuts
the tissue. This is detrimental in dental surgery because the tears that are created willcomplicate healing. In contrast, the inner curvature of a reverse-cutting needle is
smooth, with a third cutting edge located on the convex (outer) edge.4 Figure 2
illustrates the inner curvature of a reverse-cutting needle compared to a conventional
needle. For suturing of mucoperiosteal flaps in the oral cavity, the three-eighths reverse-
cutting needle with 3-0 or 4-0 thread diameters and the one-half reverse-cutting needle
with thinner 5-0 or 6-0 thread diameters are commonly used combinations.
Suture Material
Tensile strength is an important quality when determining which suture material is
appropriate for specific situations. Tissue biocompatibility and ease of handling, with afocus on minimal knot slippage, also influence which thread should be selected. The
clinician should select the suture material and diameter based on the thickness of the
tissue to be sutured and whether there is a need for flap tension. 4
Therefore, selection of the suturing technique and material should be based on the goals
of the surgical procedure and the physical/biologic characteristics of the suture material
in relationship to the healing process. Adequate strength of the suture material will
prevent breakage during suturing, and proper tying of the knot in consideration of the
material being used will prevent untying or knot slippage. The clinician must also
understand the nature of the suture material, the wound healing process, the biologic
forces exerted on the healing wound (eg, muscle pulls and swelling), and the interaction
of the suture and tissue. The suture must retain its strength until the tissues of the flaps
-
7/27/2019 Suturando para sucesso cirrgico.pdf
4/11
regain sufficient strength to keep the wound edges together. In clinical situations where
the tissues will not regain their preoperative strength, or tension is exerted on the
surgical flaps, consideration should be given to using a suture material that retains long-
term strength (up to 14 days) and resorbs in 21 to 28 days, such as conventional
polyglycolic acid (PGA) suture material.2,4 A clinical example would be a resorbed
anterior mandible that has muscle attachments close to the crestal ridge; when the flapmargins are reapproximated there will be tension on the margins. Should a resorbable
suture material be used that loses its tensile strength after a few days, the re-adhesion of
the periosteum to the underlying bone will not have gained enough strength to
overcome the muscle pull. Therefore, a longer-lasting suture material should be utilized
until the flap has achieved sufficient reattachment to the bone.
Resorbable sutures lose tensile strength over a period of time from several days to
several weeks, and the breakdown of the resorbable material should equal the healing
rate of the tissue being coapted by the material. If a suture is to be placed in tissue that
heals rapidly, a resorbable suture should be used that will lose its tensile strength at
approximately the same rate as the tissue gains strength. The suture will be absorbed bythe tissue, leaving no foreign material in the wound after healing. Examples are surgical
gut or the rapidly resorbable PGA sutures (PGA-FA).1
Resorbable sutures re-sorb due to 2 mechanisms. Sutures of biological origin (eg,
surgical gut, plain and chromic gut) are gradually digested by enzymes in the tissue,
whereas resorbable sutures fabricated from synthetic materials such as polygycolic acid
are hydrolyzed via the Kreb's cycle.2 Surgical gut suture material is made from animal
protein (ie, gut), thus it can potentially induce an antigenic reaction.6 When used
intraorally, this material loses most of its tensile strength in 24 to 48 hours; coating the
material with a chromic compound extends resorption to 7 to 10 days, and extends
significant tensile strength to 5 days.5
An additional consideration with regard to gut su-tures is that breakage of the material
during the resorption process may occur too rapidly to maintain flap apposition,
particularly if used in patients with a very low intraoral pH.4 Many physiological events
can cause a decrease in intraoral pH, including disorders such as epigastric reflux, hiatal
hernia, and bulimia. Sjogren's syndrome, chemotherapy, radiation therapy, and certain
medications (eg, angiotensin-converting inhibitors, anti-psychotics, diuretics,
antihypertensive agents, antipsoriasis medications, and steroid inhalers) can cause
xerostomia and a low intraoral pH.2,7
Coaptation of tissue flaps requires a minimum of 5 days.5 Selection of a fast-absorbing
PGA suture is indicated in clinical situations where there is a low intraoral pH (and
surgical gut sutures are contraindicated). PGA-FA suture material is not affected by low
intraoral pH; it is manufactured from synthetic polymers and is mainly degraded by
hydrolysis in tissue fluids (via enzymes involved in the Kreb's cycle). This requires 7 to
10 days.1,2 This material has a higher tensile strength than surgical gut suture material,
but its resorption rate is comparable to that of surgical gut sutures under normal
intraoral physiologic conditions.1,2
Nonresorbable sutures are fabricated either from natural or synthetic materials. Silk has
been the most widely used material for dental and many other types of surgery.8
Silk iseasy to handle, is tied with a slipknot, and costs less than many other nonresorbable
-
7/27/2019 Suturando para sucesso cirrgico.pdf
5/11
suture materials. However, silk sutures have certain disadvantages. Being nonresor-
bable, silk sutures must be removed by the clinician, usually 1 week following surgery.
The patient generally is not anesthetized for this suture removal. Further, being a
multifilament thread, silk demonstrates a "wick effect," which pulls bacteria and fluids
into the wound site.9 Therefore, silk is not the suture material of choice when foreign
materials such as dental implants, bone grafts, or regenerative barriers are placed undera mucoperiosteal flap, or when infection of the surgical site is present at the time of
surgery (ie, removal of a septic tooth).
Nonresorbable sutures that can be used in situations where silk is contraindicated
include nylon, polyester, polyethylene, polypropylene, or expanded
polytetrafluoroethylene (e-PTFE). Polyester sutures comprise multiple filaments of
polyester polymer, which are braided into a single strand that possesses high tensile
strength and does not weaken when moistened. A biologically inert, nonresorbable
compound of proprietary composition4 is often used to coat these sutures to aid the
suture in passing more easily through tissues. However, this coating allows the material
to untie easily unless the suture is secured with a surgeon's knot. 4 Nonresorbable e-PTFE suture material is a monofilament with high tensile strength, good handling
properties, and good knot security. It is, however, expensive compared with other
nonresorbable suture materials.1
Table 2. Suture Thread Types Used in Dentistry.
(A) Nonresorbable
Type Commonly used thread size
silk 3-0, 4-0, 5-0
nylon 4-0, 5-0, 6-0
polypropylene 5-0, 6,0
e-PTFE 4-0, 5-0
(B) Resorbable
Type Commonly used thread
size
Resorption time
(days)
gut 4-0 3 to 5
chromic gut 4-0, 5-0 7 to 10
PGA 3-0, 4-0, 5-0 21 to 28
PGA-dyed 3-0, 4-0, 5-0 21 to 28
In addition to material composition, surgical threads are also classified by numbering
from 1 to 10; higher numbers indicate thinner, more delicate thread.10 For example, in
implant dentistry a 3-0 thread diameter is generally used to secure flaps when a mattress
suturing technique is used, and a 4-0 thread is used closer to the flap edges to coapt
tension-free flap edges. A 4-0 thread also is used to secure implant surgical flaps when
interrupted sutures, horizontal or vertical mattress sutures (depending on where the
tissue is positioned), and most continuous suture techniques are utilized. In periodontal
plastic surgery procedures a 5-0 thread diameter is most often used to secure soft-tissue
-
7/27/2019 Suturando para sucesso cirrgico.pdf
6/11
grafts and transpositional/sliding pedicle flaps. When securing most other periodontal
mucoperiosteal flaps, 4-0 thread is used (Table 2).
SURGICAL KNOTS
Figures 3a to 3c. Slipknot
being tied.
3b.
3c. Figures 4a to 4c. Surgeon's
knot being tied.
4b. 4c.
Tying surgical knots is a critical aspect of suturing. The appropriate surgical knot
should be used for the specific suture material in order to ensure knot security. For
example, a slip (granny) surgical knot, which allows the surgeon to tighten the suturetoward the tissue without loosening or opening, could be used for e-PTFE, chromic gut,
or plain gut suture material (Figures 3a to 3c). However, a surgeon's knot, which will
remain where positioned, must be used with synthetic resorbable and nonresorbable
suture materials to prevent untying of the knot4 (Figures 4a to 4c). The mode of
manufacture of each specific suture thread determines the type of knot that is used. 5
-
7/27/2019 Suturando para sucesso cirrgico.pdf
7/11
EXAMPLES OF USEFUL SUTURING TECHNIQUES
Figure 5. A simple loop suture
used to coapt flap margins.
Figure 6. The simple loop
suture being tied to coapt the
edges of the incision.
Two suturing techniques can be used for the interrupted suture: the simple loop and thecriss-cross (which is a modification of the horizontal mattress suture technique). In
dental surgery, the simple loop (Figure 5) is used most commonly to coapt tension-free,
mobile surgical flaps.4 Procedures where the simple loop is useful include surgery of
edentulous ridge areas, to coapt vertical releasing incisions, for periosteal suturing, and
to coapt flaps as part of certain periodontal surgical procedures (ie, modified Wid-man
flap, some periodontal regeneration surgery, and some exploratory flap procedures). A
simple loop is created by entering the buccal flap from the epithelial surface (position 1)
and crossing under the periosteum to exit the epithelial surface of the lingual flap
(position 2); a knot is tied toward the buccal (Figure 6). (Note: This example assumes a
simple flap where all the soft tissue has been elevated off the bone, including the
periosteum.)
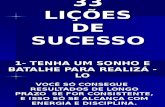
Figure 7. A criss-cross suture
placed at an extraction site toclose the margins and aid in
retention of graft material
placed in the socket.
The criss-cross is similar to the simple loop on the buccal aspect; however, on the
lingual aspect, the needle penetrates first through the epithelial surface of the lingual
flap, thus interposing additional suture thread between the surgical flaps. The criss-cross
technique is useful when suturing on the lingual aspect of the man-dibular molars,especially in a patient with an active gag reflex or a large tongue. 4 A criss-cross suture is
tied by entering the mesial buccal aspect (position 1) and exiting the distal buccal aspect
(position 2); the suture is then crossed over the socket, enters the mesial lingual aspect(position 3), and exits the distal lingual aspect (position 4). The suture at the distal
-
7/27/2019 Suturando para sucesso cirrgico.pdf
8/11
-
7/27/2019 Suturando para sucesso cirrgico.pdf
9/11
-
7/27/2019 Suturando para sucesso cirrgico.pdf
10/11
References
1. Silverstein LH. Essential principles of dental suturing for the implant surgeon.Dent
Implantol Update. 2005;16:1-7.
2. Silverstein LH. Suture selection for optimal flap closure and tissue healing. Perio-implant showcase.Pract Periodontics Aesthet Dent. 2005;16:2-3.
3. Cohen ES. Sutures and suturing. In:Atlas of Cosmetic Reconstructive Periodontal
Surgery. 2nd ed. Philadelphia, Pa: Lea & Febiger; 1994:9-30.
4. Silverstein LH.Principles of Dental Suturing: The Complete Guide to Surgical
Closure. Mahwah, NJ: Montage Media; 2000.
5. Wound Closure Manual. Somerville, NJ: Ethicon Inc; 1985:1-101.
6. Knot Tying Manual. Somerville, NJ: Ethicon, Inc; 1968.
7. Lilly GE, Salem JE, Armstrong JH, et al. Reaction of oral tissues to suture materials.
Oral Surg Oral Med Oral Pathol. 1969;28:432-438.
8. Macht SD, Krizek TJ. Sutures and suturingcurrent concepts.J Oral Surg.
1978;36:710-712.
9. Manor A, Kaffe I. Unusual foreign body reaction to a braided silk suture: a case
report.J Periodontol. 1982;53:86-88.
10. Meyer RD, Antonini CJ. A review of suture materials, part I. Compendium.
1989;10:260-265.
11. Mejias JE, Griffin TJ. The absorbable synthetic sutures. Compend Contin Educ
Dent. 1983;4:567-572.
12. Hutchens LH. Periodontal suturing: a review of needles, materials and techniques.
Postgrad Dent. 1995;2(4):1-15.
13. Silverstein LH, Kurtzman GM. A review of dental suturing for optimal soft-tissue
management. Compend Contin Educ Dent. 2005;26:163-171.
Acknowledgment
Illustrations by David Kurtzman, DDS.
-
7/27/2019 Suturando para sucesso cirrgico.pdf
11/11
Dr. Gregori Kurtzman is assistant clinical professor, University of Maryland,
Baltimore College of Dental Surgery, Department of Endodontics, Prosthetics, and
Operative Dentistry, and is in private practice in Silver Spring, Md. He can be reached
at (301) 598-3500 [email protected].
Dr. Silverstein is associate clinical professor of periodontics at the Medical College ofGeorgia in Augusta, Ga, and is author of the text Principles of Dental Suturing: A
Complete Guide to Surgical Closure. He is in private practice in Mari-etta, Ga, and can
be reached at (770) 952-5432.
Dr. Shatz is assistant clinical professor of periodontics at the Medical College of
Georgia in Augusta, Ga, and is in private practice in Marietta, Ga. He can be reached at
(770) 952-5432.
Dr. David Kurtzman is in private practice in Marietta, Ga. He can be reached at (770)
980-6336
mailto:[email protected]:[email protected]:[email protected]:[email protected]