
Practice-Relevant Focusing-Oriented Research: An Invitation / Praxisrelevante Focusing-orientierte...
20
This article was downloaded by: [The Aga Khan University] On: 09 October 2014, At: 06:38 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Person-Centered & Experiential Psychotherapies Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rpcp20 Practice-Relevant Focusing-Oriented Research: An Invitation / Praxisrelevante Focusing-orientierte Forschung: eine Einladung / Investigación orientada al focusing relevante a la práctica: Una invitación / La recherche pertinente à la pratique de l'approche Focusing: Une invitation / Investigação oientada pelo focusing de relevância pática: Um convite / James Iberg a a Evanston, Illinois, USA Published online: 06 Sep 2011. To cite this article: James Iberg (2010) Practice-Relevant Focusing-Oriented Research: An Invitation / Praxisrelevante Focusing-orientierte Forschung: eine Einladung / Investigación orientada al focusing relevante a la práctica: Una invitación / La recherche pertinente à la pratique de l'approche Focusing: Une invitation / Investigação oientada pelo focusing de relevância pática: Um convite / , Person-Centered & Experiential Psychotherapies, 9:3, 171-188, DOI: 10.1080/14779757.2010.9689065 To link to this article: http://dx.doi.org/10.1080/14779757.2010.9689065 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities
Transcript of Practice-Relevant Focusing-Oriented Research: An Invitation / Praxisrelevante Focusing-orientierte...
This article was downloaded by: [The Aga Khan University]On: 09 October 2014, At: 06:38Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office:Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Person-Centered & ExperientialPsychotherapiesPublication details, including instructions for authors and subscriptioninformation:http://www.tandfonline.com/loi/rpcp20
Practice-Relevant Focusing-OrientedResearch: An Invitation / PraxisrelevanteFocusing-orientierte Forschung: eineEinladung / Investigación orientada alfocusing relevante a la práctica: Unainvitación / La recherche pertinente àla pratique de l'approche Focusing: Uneinvitation / Investigação oientada pelofocusing de relevância pática: Um convite /James Iberg aa Evanston, Illinois, USAPublished online: 06 Sep 2011.
To cite this article: James Iberg (2010) Practice-Relevant Focusing-Oriented Research: An Invitation /Praxisrelevante Focusing-orientierte Forschung: eine Einladung / Investigación orientada al focusingrelevante a la práctica: Una invitación / La recherche pertinente à la pratique de l'approche Focusing: Uneinvitation / Investigação oientada pelo focusing de relevância pática: Um convite / , Person-Centered &Experiential Psychotherapies, 9:3, 171-188, DOI: 10.1080/14779757.2010.9689065
To link to this article: http://dx.doi.org/10.1080/14779757.2010.9689065
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”)contained in the publications on our platform. However, Taylor & Francis, our agents, and ourlicensors make no representations or warranties whatsoever as to the accuracy, completeness, orsuitability for any purpose of the Content. Any opinions and views expressed in this publicationare the opinions and views of the authors, and are not the views of or endorsed by Taylor &Francis. The accuracy of the Content should not be relied upon and should be independentlyverified with primary sources of information. Taylor and Francis shall not be liable for anylosses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities
whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantialor systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, ordistribution in any form to anyone is expressly forbidden. Terms & Conditions of access and usecan be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 171© Iberg 1477-9757/10/03171-18
Practice-Relevant Focusing-OrientedResearch: An Invitation
James Iberg
Evanston, Illinois, USA
Author Note. Address correspondence to Dr. James Iberg, 2009 McDaniel Avenue, Evanston, IL 60201-2124,USA. Email: [email protected]
Abstract. A quality improvement method, the factorial experiment, is proposed for researching focusing-oriented psychotherapy. This involves practitioners as researchers into their own practices – makingsmall activity changes and assessing effects. A sample study is described to illustrate the approach. Focusing-oriented therapists are invited to join in such a study, and first steps toward that end are described.
Keywords: practitioner-researcher, psychotherapy research, focusing, quality improvement, factorialexperiment, empathic reflecting
Praxisrelevante Focusing-orientierte Forschung: eine EinladungEs wird eine Methode zur Qualitätsverbesserung, das Faktorenexperiment, vorgeschlagen, um Focusing-orientierte Psychotherapie zu erforschen. So werden Praktikerinnen und Praktiker als Forschende inihrer eigenen Praxis einbezogen – sie machen kleine Aktivitätsveränderungen und werten die Auswirkungenaus. Eine Fallstudie wird beschrieben, um das Vorgehen zu illustrieren. Focusing-orientierteTherapeutinnen und Therapeuten sind eingeladen, bei einer solchen Studie mitzumachen und ersteSchritte auf dieses Ziel hin werden beschrieben.
Investigación orientada al focusing relevante a la práctica: Una invitaciónSe propone un método para mejorar la calidad, el experimento factorial, para investigar la psicoterapiaorientada al focusing. Esto implica a los profesionales como investigadores de sus propias prácticas –realizando cambios pequeños en su actividad y evaluando los efectos. Describimos un caso de estudiopara ilustrar este enfoque. Invitamos a los terapeutas orientados al focusing a sumarse a este estudio, ydescribimos los primeros pasos para encaminarse a esta propuesta.
La recherche pertinente à la pratique de l’approche Focusing: Une invitationUne méthode d’amélioration qualitative, l’expérience factoriale, est proposée pour la recherche dans lapsychothérapie dans l’approche Focusing. Elle implique les praticiens en tant que chercheurs par rapportà leurs propres pratiques – faisant des petits ajustements dans leurs réponses et évaluant les effets produits.Un exemple d’étude est décrit pour illustrer l’approche. Les thérapeutes dans l’approche Focusing sontinvités à rejoindre une telle étude, et les premiers pas dans ce sens sont décrits.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

172 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
Investigação oientada pelo focusing de relevância pática: Um conviteÉ proposto um método de melhoria de qualidade para o estudo da psicoterapia orientada pelo focusing,a experiência factorial. Implica os técnicos como investigadores na sua prática clínica – introduzir pequenasmudanças de actividade e avaliar os efeitos. É descrito um estudo como amostra ilustrativa dessa abordagem.Convidam-se os terapeutas orientados pelo focusing e descrevem-se os primeiros passos com vista a essefim.
Rogers (1957) argued that therapist positive regard, genuineness, and empathy are essentialfor desirable outcomes in psychotherapy. The importance of these therapist contributionshas been shown in various treatment approaches (Bohart, Elliott, Greenberg, & Watson,2002; Watson & Geller, 2005). Focusing-oriented therapists believe one way these thingsoperate is by fostering and supporting client focusing.
The term focusing was chosen by Gendlin (1969, 1981) to describe a collection ofintrospective movements and attitudes that were associated with greater progress inpsychotherapy (Gendlin, Beebe, Cassues, Klein, & Oberlannder, 1968). Focusing involvesself-empathy: a therapeutic relationship with one’s inner experiencing (Cornell, 2005; Gendlin,1984). The focuser spends time sensing viscerally, with accepting attitudes, the meaning ofsituations; sensing what more is felt than is easily understood and symbolized. Hendricks(2001) reviewed research supporting the claim that focusing is related to good outcomes.People are trained as focusing teachers and therapists in over 40 countries. Focusing-orientedpsychotherapy is a term for therapy conducted by therapists from a variety of theoreticalorientations who consider focusing to be an essential activity in psychotherapy (Gendlin,1996). The purpose of this paper is to promote a round of research on focusing-orientedpsychotherapy.
The approach suggested here borrows from practical applications of science inmanufacturing, namely, quality improvement methods (Berwick, 1989; Deming, 1986; Juran,1979; Roberts, 1988, 1989). One starts with ongoing processes and applies statistical methodsto see if improved results can be generated with small adjustments in the way things are done.We hope to start with therapists in their natural setting operating as they feel most effectivelyresponsive to clients. Experienced focusing-oriented therapists (FOTs) have response typesused regularly that they believe to facilitate focusing. Stiles (1999, p. 7) stated: “If therapistsrespond appropriately to client requirements for a particular process component (e.g.,interpretations), then each client will tend to get the optimum amount at the optimum time.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 173
It wouldn’t help to get more or less.” In this paper I propose and illustrate a design for testingwhether or not it helps to give the client more or less of some process components. Perhapswe can enhance responsiveness by investigating the effects of subtle shifts in the averageamounts of specified types of response.
As the more successful automakers have discovered, any process, no matter how much ithas been improved in the past, can be further improved. Most practicing therapists have theoccasional client with whom their usual way of being responsive fails to get the usual level ofoutcome. And even if a therapist’s usual way of being responsive achieves good outcomes fora particular client, it remains a possibility worth testing that therapeutic benefits achieved inthat therapy dyad could be increased further by systematic changes in the levels of some ofthe therapist’s activities. In discovering what improves outcomes in particular dyads, we mayeven discover that some such changes are likely to benefit many therapeutic dyads.
Many variables other than the cues in the immediate interaction affect how a therapistresponds. One is the therapist’s preconception of the best blend of therapist activities derivedfrom training and past experience. It is possible that improvements in a therapist’s responsivenessto a particular client can be made if we study that process in an effective way. Qualityimprovement process studies could help therapists continue to develop responsiveness, andcombat the tendency to become creatures of habit.
We may be able to identify a few types of response used by each of several FOTs. Forexample, since many use a lot of empathic responding, we might ask “How often should thetherapist give empathic responses?” Similarly, many FOTs give invitations to the client tofocus. What is a fruitful pace for making focusing invitations?
We will describe a completed study of the kind proposed to illustrate how such studieswork and the kinds of results produced. Such studies are well suited to learning what improvesresults for particular therapists with particular clients. They can sometimes be more broadlyinformative of what is likely to be effective in general in actual practice (the second and thirdtypes of question pursued in researching psychological treatment, described by Howard,Moras, Brill, Martinovich, and Lutz, 1996).
One particular quality improvement methodology is suggested and illustrated below:factorial experiments with two-level independent variables.
TWO-LEVEL ACTIVITY VARIABLES
Norcross (2002, p. 5) commented that “… although most treatment manuals mention theimportance of the therapy relationship, few specify what therapist qualities or in-sessionbehaviors lead to a curative relationship.” Horvath (2005) suggested that we will gain fromidentifying therapist activities associated with positive or improving alliances. Examiningspecific therapist activities is a more precise way of defining therapist behavior than adherenceto a treatment manual. Researching specific therapist activities may increase precision aboutwhat we mean by “empathic,” “genuine,” or “accepting.”
If we identify two or three shared specific activities our therapists believe to bear on
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

174 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
focusing, each activity can be considered in terms of its incidence in existing practice. Forexample, how often per session do therapists give a focusing invitation? Once the level alreadyin use is estimated, we can explore a modest variation from that level, a little more or a littleless, for two levels, to compare. Testing only two levels at a time facilitates learning whilemaking only very small adjustments from ongoing practice. Over multiple studies, more ofthe full range of levels for each activity can be explored, using the superior level found in onestudy as one of the two levels examined in the next study.
The two-level concept is actually very broad: two activities not on a conceptual continuumcan also be contrasted with each other. For example, the two levels compared might befocusing guidance in the form of questions (interrogative) vs. in the form of suggestions(declarative). Another contrast could be sessions starting with clearing a space (Gendlin, 1981;Katonah, 1999) vs. starting without that. Activity variables and levels should be chosen thatare pertinent to the clinical situation being studied.
FACTORIAL EXPERIMENTS
A factorial experiment is designed so that experimental variables (activity variables) areorthogonal, as are their interactions. Hence, in relatively few sessions, one can detect statisticallysignificant main effects for each variable, as well as effects produced by interactions betweenvariables. Each therapist involved in the study completes the entire experiment, so that resultsunique to one individual therapist can be detected, as well as results applying across allparticipating therapists, if present. This will become clearer through the study describedbelow.
METHOD
A factorial experiment
The study reported here illustrates an experiment with three two-level therapist activities. Itwas conducted with students in a basic client-centered and experiential psychotherapy (CCEP)class in a Midwestern U.S. graduate school. The three therapist activities were: asking questions,making an evaluative comment, and two frequencies of empathic responding. These weredesigned into a factorial experiment (Box, Hunter, & Hunter, 1978). The whole experimentwas completed by each therapist–client dyad. Postsession questionnaires assessed immediatesession outcome. Students applied all blends of these three therapist activities, to learn frompractice clients’ session reports about their effects.
Each activity was tested at levels close to what students already were doing. Thus, thestudy was naturalistic, not requiring therapists to learn or do things dramatically differentfrom existing repertoires, and not subjecting clients to dramatic variations in therapist activity.With three two-level activities, there are eight (2 x 2 x 2) distinct blends.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 175
Hypotheses
The first hypothesis, based on the findings of earlier studies (Iberg, 1991, 1996) and client-centered theory, was that there would be advantages to more frequent empathic responses(i.e., a main effect for frequency of empathy).
A second hypothesis was that there would not be one unique combination (blend) oftherapist activities superior to all others, such as more frequent empathy, no questions, andno advice. Rather our prediction is that sets of activity combinations sharing the same level ofa factor would show superiority: i.e., main effects would be more prevalent than higher-orderinteractions. Thus we expect to find that blends sharing higher frequency of empathy willproduce better outcomes, and that we may find advantages to blends having in common onelevel of another factor, but we don’t expect to find better outcomes limited to more complexcombinations requiring one level of a factor to be combined with a certain level of another orboth other factors.
The second hypothesis seemed more plausible than the one implied by some classicalteachers of client-centered therapy. Their hypothesis seemed to be that the best results forstudent therapists would come from one blend of therapist activity: ask no questions, makeno evaluations, and provide many empathic responses. For one of eight activity blends to besuperior to all others would require a significant three-way interaction. We tested this blendof therapist activity along with variations involving one opportunity for the therapist to ask aquestion, and one opportunity for therapists to make an evaluative response. Empathicresponses were tested at a relaxed pace, as student therapists had used in practice, vs. a higherfrequency, approximating the pace Rogers used with Gloria (Shostrum, 1966).
We explored effects of the activities on one session-level focusing outcome: an index ofthe amount of opening up of client feelings.
Participant dyads
TherapistsTherapists were five graduate students at a professional school of psychology, average age25.8, four female, one male. Three had present or prior work experience with inpatientpopulations, two had minimal clinical experience. Three were single, two married.
ClientsStudent therapists each found a volunteer client outside class who was interested and willingto serve as a practice client for ten weekly sessions. All five were female; three in their twenties,two in their forties. Two reported prior therapy, three reported never having had therapy.Occupations were student nurse, teacher, caseworker with foster children, healthcareconsultant, and unknown. Although not a clinical sample, it was representative of practiceclients in numerous sections of the course.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

176 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
Treatments
We studied: (1) Frequency of Questions contrasting two very low levels: therapist refrains fromasking questions from his/her frame of reference throughout the session vs. therapist can askone such question about a third of the way through; (2) Frequency of Evaluations, alsocontrasting two very low levels: therapist refrains from stating evaluation entirely vs. therapistmakes one evaluative comment about two-thirds of the way through; and (3) Frequency ofEmpathy: therapist gives an empathic response about every 1–2 minutes (lower frequency)vs. about every 30 seconds (higher frequency). The eight combinations (blends) of therapistactivity are detailed in Table 1.
Questions, as tested here, are those initiated from the therapist’s frame of referenceinquiring about client’s experience (Stiles, 1999). An example of a question used by onestudent therapist is: “To what extent do you feel that your father’s past drinking problem hasinfluenced your current feelings toward him?”
Evaluations are interpretations initiated from the therapist’s frame of reference concerningthe client’s experience. An example evaluation: “Well, I don’t think he would have been withyou if he didn’t want to be with you.”
Empathy was operationalized as paraphrasing and saying back the meaning, from theclient’s point of view, that the client had just expressed. A session segment illustrating such aresponse follows:
C: I mean, it’s helped, me talking to you, ’cause I’m able to get it out and, umm, you know, it,it just helps talking to somebody about what I’m feeling. It almost, it’s just a tension releasefor me.
T: So you feel better being able to get it off your chest and talk about it.
Each dyad completed ten sessions. The first two were baseline sessions with the instructions weused to start students learning client-centered therapy: ask no questions, make no evaluations,and give plenty of empathic responses. Students had been coached to practice this way duringclassroom exercises. Thus, baseline sessions were roughly the blend of Treatment 1.
Table 1. Treatments: The Eight Possible Blends of Our Three Two-Level Therapist Activities
Treatments Frequency of:Questions Evaluation Empathy
1 None None Lower
2 Ask one None Lower
3 None One Lower
4 Ask one One Lower
5 None None Higher
6 Ask one None Higher
7 None One Higher
8 Ask one One Higher
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 177
Procedure
After two baseline sessions, each dyad completed eight weekly study sessions, one for eachtreatment. The order of the eight treatments was randomized within dyad, to control foreffects associated with the passage of time and cumulative experience: thus, each therapistapplied the eight blends of activity in a different chronological order.
Materials
Client Postsession QuestionnaireImmediately after each session, practice clients filled out an early version of The Focusing-oriented Session Report (the FSR; Iberg, 2002). Factor analysis suggested several index variables,one of which, called Opening, was selected as an indicator of the quality of the focusing inthe session.
Outcome measureThe index variable Opening of Feelings/Actuality of Trust (Opening) is the sum of standardizedscores on five items (each item with an anchored Likert scale of possible responses):
“Opening” Subscale Items• To what extent did the “doorway” to your feelings open in this session?
• How well did your listener seem to understand what you were feeling and thinkingthis session?
• To what extent do you feel you were able to talk about what was valuable for youto discuss?
• Please rate the following two aspects of the emotional intensity of the session:(a) How intense was the most intense emotion you felt?
(b) Sometimes people keep their more intense feelings to themselves for variousreasons. How much of this session was spent talking about or openly expressingthe most intense emotions you felt?
Item scores were standardized so they had: means = 0 and standard deviations = 1. Standardizedscores were summed to create the index variable Opening.
Cronbach’s coefficient alpha, a measure of internal consistency, is theoretically an indicatorof a measure’s correlation with true scores on the underlying variable. Alpha on this samplewas .56. This is lower than we would like, but for a new instrument it is in the acceptablerange (Nunnally, 1967, p. 226). Later versions of the FSR (developed since this study wascompleted) have additional items for Opening, which improves reliability.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

178 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
Therapist instructions
After two baseline sessions and prior to the eight experimental sessions, student therapistsreceived written descriptions of the three activity factors (available on request). There wasclass discussion for clarification before study sessions began. In an effort to preserveresponsiveness during execution of the experiment, written instructions concluded as follows:
Overall: it is very important, if we are to obtain meaningful results, that you do varyyour therapist activities as well as you can, according to the instructions. At the sametime, the more important purpose of all of the sessions is to give each client a highquality experience of being understood empathically with respect and genuineness.If it should ever happen during a session that you feel staying with the instructionswould seriously reduce the quality of the session for the client, then do what youneed to do to maintain the quality of the session. If you can return to the instructionsa little later, please do, but the client’s interest comes first.
Before each experimental session, students received a note with the specific activity combinationto be used in that session. Each student had a small clock to keep in view to help paceempathic responses, and to help place the question and the evaluation. Empathic responseswere not to be rigidly given by the clock, but a pace approximating the assigned level was tobe strived for.
Statistical design: 23 factorial experiment
Pre-study sessions were coded “0” on the activity factors. Each activity variable in theexperimental sessions was coded “–1” and “+1” for the two experimental levels. This codingmeans that we are statistically testing the significance of the two levels of an activity for effectsdiverging from pre-study outcome levels.
By randomizing the order of treatment within each of the five therapist–client dyads,we controlled for unmeasured influences on outcomes correlated with the passage of time,such as practice effects or simple familiarity within the dyad.
Manipulation checks: Validating experimental variations in therapist activity
The primary source of data for verifying that the experiment occurred as intended was clientestimates of therapist behavior. Three questions were added to postsession questionnaires:One queried whether the listener asked any questions during the session, with a yes or noanswer. Another asked if the listener made any judgments or evaluative remarks, or expressedapproval or disapproval, also with a yes or no answer. The third asked for a rating of frequencyof understanding responses on a five-point scale from “less often than every five minutes,” to“more often than every 30 seconds.”
A secondary source of manipulation-check data was audiotapes of 5–10 minute sectionsof the sessions, also transcribed, that were turned in for assignments. These included, for
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 179
every session that included them, therapist questions and therapist evaluations, and theyincluded examples of both levels of empathic responding. With these, questions asked andevaluative comments made were examined, and frequencies of empathic response wereestimated by the author and compared to assigned levels.
RESULTS
Validation of experimental activity variations
Client estimates validated that therapists adjusted their behavior according to the assignedconditions of the experiment. For example, client estimates of the rate of empathic respondingduring the pre-study level clustered around “once every couple of minutes”; estimates for thehigher rate clustered around “about once every 30–60 seconds”; and estimates of the lowerrate clustered around “once every 3–5 minutes.”
Client estimates were regressed on the assigned levels of the experimental variables,which confirmed that assigned levels were corroborated by client estimates both in convergent(p < .001 in each case) and discriminant ways (no cross-correlation with p < .26).
A count of frequencies of empathic response from the taped five-minute segmentsindicated sample averages for the lower frequency of one every 62 seconds, and for the higherfrequency of one every 37 seconds.
Variables for regression analysis
Five dyads each conducted two practice sessions and then eight sessions according toexperimental requirements, so there were ten sessions for each dyad, and a total of 50 sessions.In one baseline session for Dyad 1, the client gave no answer on one or more of the items inthe Opening index variable, so that was treated as a missing value. Hence, we have 49Opening scores.
There are three experimental variables (whether or not therapists asked a question; whetheror not the therapist made an evaluation; and lower or higher frequency of empathicresponding). There are three variables for two-way interactions between experimental variables,and one three-way interaction variable (for a total of seven experimental variables). To test forlevel differences in Opening between an individual dyad and the overall mean of Opening,we represented the five dyads with four indicator variables (effects coded, see Cohen &Cohen, 1983). Finally, multiplying the indicator variables by the seven experimental variablesgenerates 28 more variables to test for experimental effects specific to particular dyads.Altogether, this produces 39 independent variables for regression analysis (see Table 2).
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014
180 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
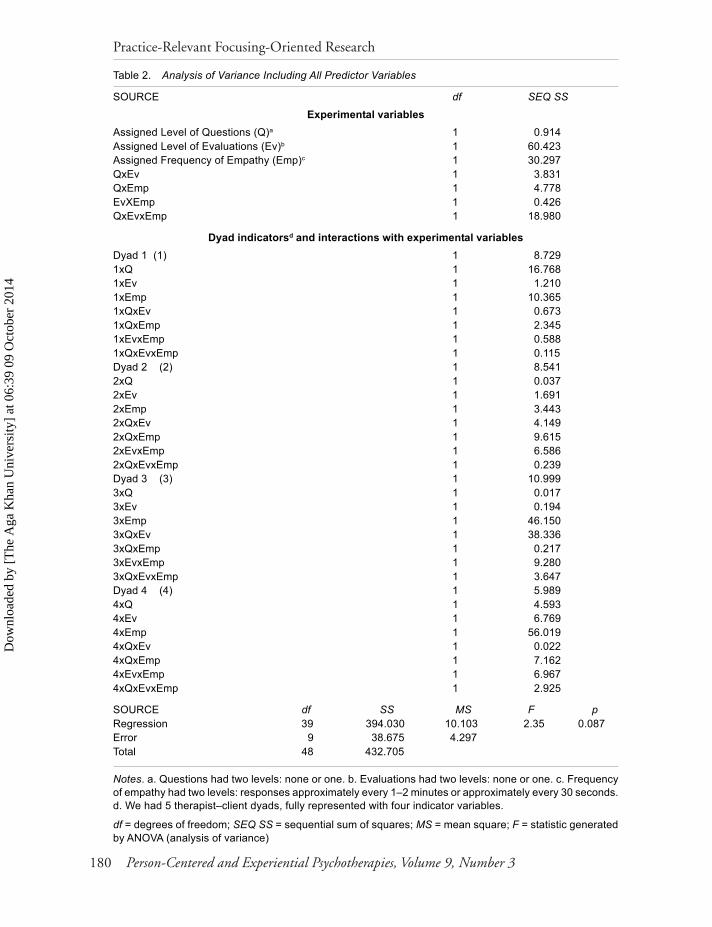
Table 2. Analysis of Variance Including All Predictor Variables
SOURCE df SEQ SS
Experimental variablesAssigned Level of Questions (Q)a 1 0.914Assigned Level of Evaluations (Ev)b 1 60.423Assigned Frequency of Empathy (Emp)c 1 30.297QxEv 1 3.831QxEmp 1 4.778EvXEmp 1 0.426QxEvxEmp 1 18.980
Dyad indicatorsd and interactions with experimental variablesDyad 1 (1) 1 8.7291xQ 1 16.7681xEv 1 1.2101xEmp 1 10.3651xQxEv 1 0.6731xQxEmp 1 2.3451xEvxEmp 1 0.5881xQxEvxEmp 1 0.115Dyad 2 (2) 1 8.5412xQ 1 0.0372xEv 1 1.6912xEmp 1 3.4432xQxEv 1 4.1492xQxEmp 1 9.6152xEvxEmp 1 6.5862xQxEvxEmp 1 0.239Dyad 3 (3) 1 10.9993xQ 1 0.0173xEv 1 0.1943xEmp 1 46.1503xQxEv 1 38.3363xQxEmp 1 0.2173xEvxEmp 1 9.2803xQxEvxEmp 1 3.647Dyad 4 (4) 1 5.9894xQ 1 4.5934xEv 1 6.7694xEmp 1 56.0194xQxEv 1 0.0224xQxEmp 1 7.1624xEvxEmp 1 6.9674xQxEvxEmp 1 2.925
SOURCE df SS MS F pRegression 39 394.030 10.103 2.35 0.087Error 9 38.675 4.297Total 48 432.705
Notes. a. Questions had two levels: none or one. b. Evaluations had two levels: none or one. c. Frequencyof empathy had two levels: responses approximately every 1–2 minutes or approximately every 30 seconds.d. We had 5 therapist–client dyads, fully represented with four indicator variables.
df = degrees of freedom; SEQ SS = sequential sum of squares; MS = mean square; F = statistic generatedby ANOVA (analysis of variance)
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 181
Experimental effects on focusing outcome
Opening of Feelings/Actuality of Trust IndexTable 2 shows the sequential sums of squares for the complete regression of Opening on theset of 39 independent variables. Many variables contribute very little to explained variance,essentially being random in effects on Opening. To find a simpler model including only thevariables with important effects on Opening, stepwise regression was performed with Openingas the dependent variable, and these 39 independent variables. This procedure examinesvariables one by one, entering or removing them according to an F-test (F to enter = 4, F toremove = 4), resulting in a much simpler model including only significant contributors toOpening variance. The model has four independent variables: Therapist Evaluations;Frequency of Empathic Responses; an interaction between Dyad 3 and Frequency of EmpathicResponses; and an interaction between Dyad 4 and Frequency of Empathic Responses(summarized in Table 3).
Higher frequency of empathic responding resulted in more Opening, and lower frequencyin less, on average, relative to pre-study sessions. Similarly, an evaluative comment made bythe therapist resulted in more Opening, and not making such a comment in less, relative topre-study sessions. These results were further specified for two dyads. For Dyad 3, the effectof the different levels of empathic responding was even stronger than for the average dyad.But for Dyad 4, the effect for the rate of empathic responding was reversed. For Dyad 4,Opening was higher for sessions with the lower rate of empathic response, and lower forsessions with the higher level.
There were no effects on Opening differentiating the levels of Questions tested frompre-study levels.
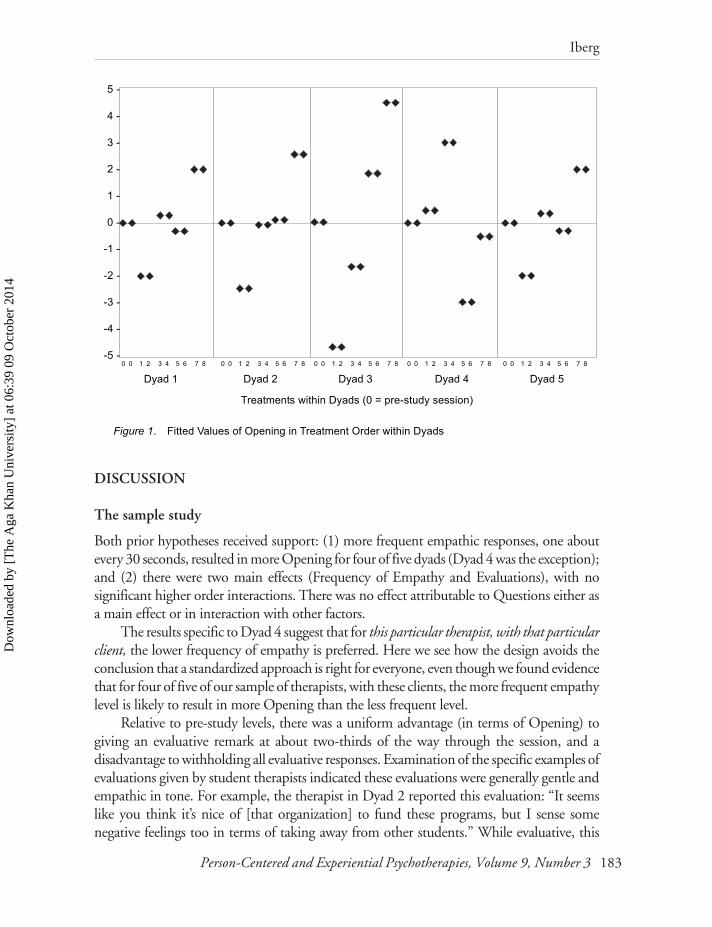
These results may be easier to grasp by examination of Figure 1, displaying fitted valuesfrom the regression model organized not in chronological order (which was randomized foreach dyad). In Figure 1, there are ten model fits for each dyad, each in the same order: twopre-study sessions followed by the treatment sessions 1–8 (from Table 1).
Table 3. Opening of Feelings/Actuality of Trust Regressed on Four Independent Variables
Regression equation: Opening = .02 + .87 Empathy + 1.23 Evaluation + 2.19 Dyad3xEmpathy – 2.62 Dyad4xEmpathy
Predictor Coefficient SD t-ratio p
Constant 0.0202 0.3385 0.06 0.953Assigned level of Empathy 0.8703 0.3747 2.32 0.025Assigned level of Evaluations 1.2291 0.3747 3.28 0.002Dyad 3 x Empathy 2.1893 0.6841 3.20 0.003Dyad 4 x Empathy -2.6235 0.6841 -3.84 0.000
R2 = 42.9%, p < .001, N = 49 (1 missing pre-study observation)
The pattern is roughly the same for four of five dyads. Average Pre-study Opening is ourreference level. Thus, the first two points for each dyad are approximately 0. Fitted values
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

182 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
during the experiment appear in groups of two corresponding to two levels of Questions,which did not predict outcome in these data. Treatments 1–4 are at the lower level of empathicresponding, and 5–8 are at the higher level. The main effect of frequency of empathic responseis seen by the fact that, with the exception of Dyad 4, the average of fitted Opening values fortreatments 1–4 is lower than the average for treatments 5–8. Average fitted value of Openingfor lower frequency sessions is below the pre-study level, and average fitted value for higherfrequency sessions is above the pre-study level. For Dyad 4, lower frequency empathy sessionshave an average fitted Opening above pre-study levels and higher frequency empathy sessionshave an average fitted Opening below pre-study levels.
The main effect for therapist evaluations is seen in that for every dyad, the average offitted Opening values for treatments 1, 2, 5, and 6 (no evaluation), is lower than the averagefor treatments 3, 4, 7, and 8. Average fitted Opening for no-evaluation treatments is belowpre-study levels and for treatments with one evaluation is above pre-study levels.
Some treatments have the more beneficial level of one activity with the less beneficiallevel of the other activity. Some have the more beneficial levels of both together, and somehave the less beneficial levels together. Treatments 1 and 2 involved the lower frequency ofempathic responding and no therapist evaluations, and these points are the lowest in eachpanel except Dyad 4, for which they are about the same as pre-study levels.
Treatments 3 and 4 involved the lower level of empathy and a therapist evaluation. Thepositive effect of therapist evaluation overcomes the negative effect of lower frequency ofempathy, maintaining Opening for these two treatments at approximately baseline level foreveryone except Dyads 3 and 4. For Dyad 3, the larger than average negative effect of lowerrate of empathic response is not made up by the beneficial effect of evaluation. For Dyad 4,the positive effect of lower level of empathy and the positive effect of a therapist evaluationcombined to make activity blends 3 and 4 the best in terms of Opening.
Treatments 5 and 6 involved higher frequency of empathy and no evaluation. Here thegeneral pattern is that Opening was near pre-study levels, except for Dyads 3 and 4. ForDyad 3, whose empathic response effect was greater than average, these two sessions haveOpening about the same level as the best of all the sessions for the other therapists. For Dyad4, the negative effect of the higher level of empathy and the negative effect of no therapistevaluation combine to make these two sessions for Dyad 4 quite low in Opening, the worstfor that Dyad.
Treatments 7 and 8 are sessions with both higher frequency of empathy, and a therapistevaluation, and for four of the five dyads, these were the most facilitative of Opening. ForDyad 4, the effects of evaluation and higher empathy offset each other so that the model fitswere about at pre-study levels.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014
Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 183
DISCUSSION
The sample study
Both prior hypotheses received support: (1) more frequent empathic responses, one aboutevery 30 seconds, resulted in more Opening for four of five dyads (Dyad 4 was the exception);and (2) there were two main effects (Frequency of Empathy and Evaluations), with nosignificant higher order interactions. There was no effect attributable to Questions either asa main effect or in interaction with other factors.
The results specific to Dyad 4 suggest that for this particular therapist, with that particularclient, the lower frequency of empathy is preferred. Here we see how the design avoids theconclusion that a standardized approach is right for everyone, even though we found evidencethat for four of five of our sample of therapists, with these clients, the more frequent empathylevel is likely to result in more Opening than the less frequent level.
Relative to pre-study levels, there was a uniform advantage (in terms of Opening) togiving an evaluative remark at about two-thirds of the way through the session, and adisadvantage to withholding all evaluative responses. Examination of the specific examples ofevaluations given by student therapists indicated these evaluations were generally gentle andempathic in tone. For example, the therapist in Dyad 2 reported this evaluation: “It seemslike you think it’s nice of [that organization] to fund these programs, but I sense somenegative feelings too in terms of taking away from other students.” While evaluative, this
Figure 1. Fitted Values of Opening in Treatment Order within Dyads
0 0 1 2 3 4 5 6 7 8 0 0 1 2 3 4 5 6 7 8 0 0 1 2 3 4 5 6 7 8 0 0 1 2 3 4 5 6 7 8 0 0 1 2 3 4 5 6 7 8
5 -
4 -
3 -
2 -
1 -
0 -
-1 -
-2 -
-3 -
-4 -
-5 -
Dyad 1 Dyad 2 Dyad 3 Dyad 4 Dyad 5
Treatments within Dyads (0 = pre-study session)
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

184 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
seems to be in the spirit of “empathic conjecture” (Bohart, Elliott, Greenberg, & Watson,2002). Another example from this dyad: “I think everything will work out because you’llgive the situation to someone else to take care of and it sounds like a good decision …because you fear conflict.” Although it is clearly an interpretation from the therapist’s frameof reference of the client’s experience and situation, this too has a lot of empathy in it, alongwith the optimistic prediction.
The therapist in Dyad 3 gave this example of evaluation: “It sounds as though you havea lot of faith in his abilities and intelligence and those are qualities you love him for, but itsounds as though the traits you need most, the security and stability, may not be traits thatthis person has had or will ever have.” This conveys considerable empathy to the client’sfeelings and views. The evaluation seems to be in the form of predicting the likelihood ofchange in the other person to whom the client referred. Another from this therapist was: “Itseems like the feelings you’re expressing are understandable given what you’ve said about thesituations.” That seems to exemplify what Bohart et al. (2002) called empathic affirmations,an empathic sort of evaluation.
These examples show that the form of evaluation implemented here was well anchoredin empathy, and it was only once in the session. When this is the case, perhaps the extrasomething that our therapists gave to make an evaluation enhanced the intersubjective quality(Schmid & Mearns, 2006) or the “I–Thou” quality (Buber, 1958) of the session, favorablyinfluencing client Opening.
Even though these appear to have been very empathic evaluations, client ratings ofwhether or not the therapist made evaluations did correspond very highly to when the therapistwas assigned to give an evaluation in the session and did not cross-correlate significantly withthe empathy variable, so clients distinguished the empathic and the evaluative aspects oftherapist activity.
These results do suggest that a rigid exclusion of all therapist evaluation by these studentsis likely to result in less Opening for practice clients than if one evaluation is included. Togain confidence in this result as applying beyond this particular group of student therapists,we need replications of experiments including this activity variable. If we were to conduct asubsequent study with this group of therapists, we might test one evaluative response vs. twoto conservatively further explore the effects of therapist evaluation.
Our results replicate earlier findings that higher frequency of empathic responding tendsto have advantages (although this is weakened by the fact that there was one of our dyads forwhom this effect was reversed). More experiments are needed to determine how broadly thisfinding may apply, but our results affirm the value of such further exploration.
Therapist questions at the levels tested had no effects differentiating them from pre-study sessions. Recall that this was a very minimal level of questions, none throughout thesession vs. one at about a third of the way into the session. The choice of such a minimal levelwas driven by the author’s desire to study practice as already ongoing and only slight variationsfrom that. In this beginning class on CCEP, students typically were coached to practiceempathic responses, pure and simple, not doing other things like asking questions and givingevaluations. Testing for the possible effects of allowing questions from the therapist’s frame of
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 185
reference at one point in the session was a conservative way of exploring whether it is reasonable,in terms of the client’s experience, to relax that restriction, and these results suggest it probablyis, at least in terms of Opening of feelings for the clients. Further studies could explore onequestion vs. two questions, since one caused no problems with Opening.
These data suggest four of our student therapists are likely to get better results in termsof client Opening of feelings by combining empathic responses about every 30 seconds withone evaluation initiated by the therapist late in the session (blends 7 and 8), rather thanpracticing as typically instructed in the past with blend 1 (no questions, no evaluations, withempathic responses every minute or two). Even our one therapist for whom the lower frequencyof empathy did better would not want to use blend 1 with that client, but instead either 3 or4 (lower frequency empathy with an evaluation late in the session).
This sample study produced results applying to this group of dyads in their actual(practice) clinical settings, and it also produced results specific to two of the individual dyads.Many other designs would not highlight dyads that differed from the rest, instead showingonly results significant for the whole group.
The study educated the author as a teacher of beginning students of CCEP to relax thebeginning instructions. In subsequent classes, we began practice allowing students oneopportunity to ask a question from the therapist’s frame of reference, and also encouragingthem to give an evaluation later in the session if they had one they deemed fitting.
Further questions remain to be explored: Are other outcomes affected by these activitiessimilarly or differently than Opening? When practicing with questions and evaluations allowed,do student therapists achieve, by the end of the course, the same quality or consistency in theirempathic responses? Do client symptoms improve more or less over a course of sessions dependingon frequency of empathy and whether or not questions and evaluations are included?
Limitations
For experienced clinicians, the illustrative study has oddly restrictive constraints on therapistbehavior. In terms of responsiveness, it would be more desirable to let the therapist choosethe appropriate moment for a question or evaluation. The rationale for the constraints wasspecific to the educational situation with students new to CCEP: the author wanted toinsure that students had to exercise self-restraint with a one-objective task (providing empathy)for at least 15–20 minutes before inviting the distraction of cognitively entertaining questionsto ask. The constraints were also chosen for the clients’ benefit: the author wanted to insurethat clients would feel a degree of confidence that the therapist wanted to understand theclient’s perspective before having alternative points of view introduced.
Some may say the difference between one or no questions or evaluations is not clinicallymeaningful. This may be true if one has in mind the sessions of more experienced therapists,where the therapist can deliver a definite sense of empathic understanding even while askingappropriate questions or making responsive evaluations. Were one to design a study for suchsituations, it would be more appropriate to test levels of these variables, and time theirapplication, according to the realities of the situation.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

186 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
As indicated earlier, our outcome measure, Opening, comprised of responses to fivequestions on a client postsession questionnaire, had lower internal consistency than we wouldlike. Further studies done with this measure should use later versions with more items andhigher reliability. Also, we only looked at this one measure from the client’s perspective. Itwould be valuable to include additional measures from the client’s perspective, and alsomeasures from the therapist’s perspective and from the perspective of objective judges.
Looking ahead
Even with these limitations, we see that small adjustments in activity levels made detectabledifferences in outcome. The author holds that these results demonstrate that for these studenttherapists with their practice clients, whether or not the therapists made one evaluation inthe session was clinically significant. The difference between one and no questions was notclinically significant. Perhaps more importantly than these specific results, the author hopesto have demonstrated that two-level factorial studies, designed with factors chosen byparticipating therapists as appropriate to their clinical situations, promise to help therapistsimprove clinical effectiveness.
Can we identify a group of between five and ten FOTs inspired by this kind of study tojoin forces for research on their practices? If each identifies two to three willing clients withwhom they would like to be more effective, we can launch a study.
A first step would be for each therapist to observe their own responses in ongoingpractice in order to identify four or five focusing-oriented activities enacted at least once ortwice in most sessions. In a few sessions, you can estimate how often each kind of response ismade. A short summary of these activities and when they tend to occur could be sent to thiswriter, to determine if we have two or three activities that are of shared interest, and whetherfor those activities a useful study could be designed.
My hope is that readers have glimpsed how factorial studies with two-level variables canbe minimally disruptive to one’s usual way of practicing. If we inspire practicing FOTs tocollaborate on “user-friendly” research that directly helps them be more effective therapists,and that also illuminates generally promising blends of therapist activity, we may actuallyreduce the still-wide practice–research gap.
REFERENCES
Berwick, D. M. (1989). Continuous improvement as an ideal in health care. The New EnglandJournal of Medicine, 320, 53–56.
Bohart, A. C., Elliott, R., Greenberg, L. S., & Watson, J. C. (2002). Empathy. In J. C. Norcross,(Ed.), Psychotherapy relationships that work (pp. 89–108) New York: Oxford University Press.
Box, G. E. P., Hunter, W. G., & Hunter, J. S. (1978). Statistics for experimenters. New York: Wiley.Buber, M. (1958). I and Thou. (Ronald Gregor Smith, Trans.). New York: Scribner.Cohen, J., & Cohen, P. (1983). Applied multiple regression and correlation analysis for the behavioral
sciences (2nd ed.). Hillsdale, NJ: Erlbaum.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

Iberg
Person-Centered and Experiential Psychotherapies, Volume 9, Number 3 187
Cornell, A. W. (2005). The radical acceptance of everything: Living a focusing life. Berkeley, CA:Calluna Press.
Deming, W. E. (1986). Out of the crisis. Cambridge, MA: MIT, Center for Advanced EngineeringStudy.
Gendlin, E. T. (1969). Focusing. Psychotherapy: Theory, Research, and Practice, 6, 4–15.Gendlin, E. T. (1981). Focusing (Rev. 2nd ed.). New York: Bantam.Gendlin, E. T. (1984). The client’s client: The edge of awareness. In R. F. Levant & J. M. Shlien
(Eds.), Client-centered therapy and the person-centered approach: New directions in theory, research,and practice (pp. 76–107). New York: Praeger.
Gendlin, E. T. (1996). Focusing-oriented psychotherapy: A manual of the experiential method. NewYork: Guilford.
Gendlin, E. T., Beebe, J., Cassues, J., Klein, M., & Oberlander, M. (1968). Focusing ability inpsychotherapy, personality and creativity. Research in Psychotherapy, 3, 217–241.
Hendricks, M. N. (2001). Focusing-oriented/experiential psychotherapy. In D. J. Cain & J. Seeman(Eds.), Humanistic psychotherapy: Handbook of research and practice. Washington, DC: AmericanPsychological Association.
Horvath, A. O. (2005). The therapeutic relationship: Research and theory. An introduction to thespecial issue. Psychotherapy Research, 15, 3–7.
Howard, K. I., Moras, K., Brill, P. L., Martinovich, Z., & Lutz, W. (1996). Evaluation ofpsychotherapy: Efficacy, effectiveness, patient progress. American Psychologist, 51, 1059–1064.
Iberg, J. R. (1991). Applying statistical control theory to bring together clinical supervision andpsychotherapy research. Journal of Consulting and Clinical Psychology, 59, 575–586.
Iberg, J. R. (1996). Using statistical experiments with post-session client questionnaires as a student-centered approach to teaching the effects of therapist activities in psychotherapy. In R. Hutterer,G. Pawlowsky, P. F. Schmid, & R. Stipsits (Eds.), Client-centered and experiential psychotherapy:A paradigm in motion (pp. 255–271). Frankfurt am Main: Peter Lang.
Iberg, J. R. (2002). Psychometric development of measures of in-session focusing activity: TheFocusing-oriented Session Report and the Therapist Ratings of Client Focusing Activity. In J. C.Watson, R. N. Goldman, & M. S. Warner (Eds.), Client-centered and experiential psychotherapyin the 21st century: Advances in theory, research and practice (pp. 221–246). Ross-on-Wye, UK:PCCS Books.
Juran, J. M. (1979). Quality control handbook (3rd ed.). New York: McGraw-Hill.Katonah, D. (1999). Clearing a space with someone who has cancer. The Folio: A Journal for Focusing
and Experiential Therapy, 18, 19–26.Norcross, J. C. (2002). Empirically supported therapy relationships. In J. C. Norcross (Ed.),
Psychotherapy relationships that work (pp. 3–16). New York: Oxford University Press.Nunnally, J. (1967). Psychometric theory. New York: McGraw-Hill.Roberts, H. V. (1988). Data analysis for managers with MINITAB. Redwood City, CA: The Scientific
Press.Roberts, H. V. (1989). Taguchi methods. Statistical quality and productivity improvement with
MINITAB (Chapter 16). Unpublished manuscript, University of Chicago.Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change.
Journal of Consulting Psychology, 21, 95–103.Schmid, P. F., & Mearns, D. (2006). Being-with and being-counter: Person-centered therapy as an
in-depth co-creative process of personalization. Person-Centered and Experiential Psychotherapies,5, 174–190.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

188 Person-Centered and Experiential Psychotherapies, Volume 9, Number 3
Practice-Relevant Focusing-Oriented Research
Shostrom, E. L. (Producer). (1966). Three approaches to psychotherapy [Film]. Santa Ana, CA:Psychological and Educational Films.
Stiles, W. B. (1999). Signs and voices in psychotherapy. Psychotherapy Research, 9, 1–21.Watson, J. C., & Geller, S. M. (2005). The relation among the relationship conditions, the working
alliance and outcome in both process-experiential and cognitive-behavioral psychotherapy.Psychotherapy Research, 15, 25–33.
Dow
nloa
ded
by [
The
Aga
Kha
n U
nive
rsity
] at
06:
39 0
9 O
ctob
er 2
014

















![Characterization of pervious concrete focusing on non-destructive … · 2020. 5. 26. · C1747 [26], to determine the degradation resistance of impact and abrasion pervious concrete;](https://static.fdocumentos.tips/doc/165x107/60a5b090cb21923a32723f97/characterization-of-pervious-concrete-focusing-on-non-destructive-2020-5-26.jpg)