Fracture Todo Na

of 152
-
Upload
nikki-m-arapol -
Category
Documents
-
view
220 -
download
0
Transcript of Fracture Todo Na
-
7/31/2019 Fracture Todo Na
1/152
FRACTURE
-
7/31/2019 Fracture Todo Na
2/152
ETIOLOGY
1. Direct force. When a bone is subjected to more stress than
it can absorb from an impact with a solidobject. e.g., Moving object strikes the body over the bony areas
2. Twisting.
In a twisting (torsion) fracture, an indirect
force may cause a break in a bone at alocation other than the site of the twistingforce. This type of injury is common in skiing accidents.
-
7/31/2019 Fracture Todo Na
3/152
3. Muscle contractionAnother indirect force fracture,
resulting from powerful contraction of
a muscle, may cause the muscles totear away from the bone, oftenfracturing or avulsing part of the bone
in the process.This type of injury may occur during a
grand mal seizure.
ETIOLOGY
-
7/31/2019 Fracture Todo Na
4/152
ETIOLOGY
4. Pathological fracture. Bones that have become weakened from
age or disease are easily fractured, oftenfrom just a slight movement
5. Fatigue or stress fracture. This type of injury may occur when a bone
has been subjected to repeated stress. The repeated stress of sustained running or
marching may cause stress fractures of the feetor lower extremities
Common to Soldiers and sports enthusiasts
-
7/31/2019 Fracture Todo Na
5/152
RISK FACTORS
Osteopenia (inadequate ossification) begins between ages 30 and
40
osteoblast activity declines, while osteoclast activity
remains level Usually caused by steroid use or Cushing syndrome
Release of osteoclast leads to accelerated boneresorption
Osteogenesis imperfecta
A congenital bone disease characterized by defectivecollagen production by osteoblasts
-
7/31/2019 Fracture Todo Na
6/152
RISK FACTORS
Neoplasms RANKL, a cytokine released by metastatic bone tumors,
thus promoting formation and activation of osteoclast =accelerated bone resorption
Postmenopausal estrogen loss
Remember, estrogen stimulates osteoblast activity andsynthesis of bone matrix
High-risk recreation or employment-relatedactivities (e.g., skateboarding, rock climbing)
-
7/31/2019 Fracture Todo Na
7/152
-
7/31/2019 Fracture Todo Na
8/152
CLINICAL MANIFESTATIONS4. Shortening of an extremity.
Occurs because of the contraction of the muscles that areattached distal and proximal to the fractured site
The fragments often overlap by as much as 2.5 to 5 cm (1-2inches)
5. Crepitus. Refers to the grating sensation or sound caused by the rubbing
together of fractured fragments
Testing for crepitus can produce further tissue damage andtherefore should be AVOIDED
6. Discoloration and Edema. Occur after a fracture as a result of trauma or bleeding into the
tissues
-
7/31/2019 Fracture Todo Na
9/152
CLINICAL MANIFESTATIONS
7. Neurovascular changes
Results from damage to the peripheral nervesor to the associated vascular structures
The client may complain of tingling ornumbness sensation or have no palpable pulsedistal to the fracture
8. Shock Bony fragments may lacerate blood vessels
Frank or occult hemorrhage can lead to shock
-
7/31/2019 Fracture Todo Na
10/152
DIAGNOSTIC EVALUATION
Comprehensive history taking
Radiograph (X-ray) the most common methodto makethe diagnosis of fracture.
CT SCAN used to determine fracture as well asinjury to soft tissue associated with fracture
Others:
CBC to check for a decreased (Hgb snd hct),
serum ELECTROLYTES if blood loss and extensivemuscle damage has occurred
EMG-NCV to detect nerve injury
-
7/31/2019 Fracture Todo Na
11/152
CLASSIFICATION OFFRACTURES
Bone fractures are classified by: The position of the bone ends after fracture The completeness of the break The orientation of the bone to the long axis
Whether or not the bones ends penetrate the skin
A fracture that is associated with a large amountof nerve, blood vessel, and soft tissue damage is
called a complicated fracture.
A fracture without other damage would bereferred to as an uncomplicated fracture.
-
7/31/2019 Fracture Todo Na
12/152
SPECIFIC TYPES OF FRACTURE(according to direction of the fracture line in relation to the bone's
longitudinal axis.)Linear
the fracture is parallel to the long axis of thebone
Transverse
the fracture is perpendicular to the long axis ofthe bone
-
7/31/2019 Fracture Todo Na
13/152
SPECIFIC TYPES OF FRACTURE(according to direction of the fracture line in relation to the bone's
longitudinal axis.)
Longitudinal.
A fracture line that runs along the length of, butnot parallel to, the bone's axis.
Oblique
A fracture line that slants across the bone.
-
7/31/2019 Fracture Todo Na
14/152
SPECIFIC TYPES OF FRACTURE(according to direction of the fracture line in relation to the bone's
longitudinal axis.)
Spiral
A fracture line that runs across the bone at anoblique angle and coils or spirals around the
bone.
-
7/31/2019 Fracture Todo Na
15/152
SPECIFIC TYPES OF FRACTURE(according to the condition of the bone)
Complete. The bone is completely brokenor split apart.
Incomplete. The bone is not completelysplit and part of the bone remains intact.
-
7/31/2019 Fracture Todo Na
16/152
SPECIFIC TYPES OF FRACTURE(according to the condition of the bone)
Closed In a closed, or simple fracture, there is
no break in the skin associated with the
fracture.
Open
An open, or compound fracture is one inwhich there is an open woundassociated with the fracture site.
-
7/31/2019 Fracture Todo Na
17/152
GRADING OF OPEN FRACTURE(grading of the extent of tissue damage)
Grade I Clean wound less than 1 cmlong
Grade II larger than 1 cm woundwithout extensive tissue damage;contamination is moderate
Grade III Highly contaminated, hasextensive soft tissue damage and isost severe; wound exceeds 6-8 cm
-
7/31/2019 Fracture Todo Na
18/152
-
7/31/2019 Fracture Todo Na
19/152
SPECIFIC TYPES OF FRACTURE(according to the condition of the bone)
Nondisplaced
bone ends retain their normal position
Displaced
bone ends are out of normal alignment
-
7/31/2019 Fracture Todo Na
20/152
-
7/31/2019 Fracture Todo Na
21/152
SPECIFIC TYPES OF FRACTURE(according to the condition of the bone)
Depressed
A piece of bone is driven inward, as in a skullfracture.
-
7/31/2019 Fracture Todo Na
22/152
SPECIFIC TYPES OF FRACTURE(according to the condition of the bone)
Comminuted
bone fragments into three or more pieces
common in the elderly
-
7/31/2019 Fracture Todo Na
23/152
SPECIFIC TYPES OF FRACTURE(according to the condition of the bone)
Greenstick
incomplete fracture where one side of the bonebreaks and the other side bends
common in children
-
7/31/2019 Fracture Todo Na
24/152
FRACTURE REPAIR
STEP 1
Bleeding:
produces a clot (fracturehematoma)
establishes a fibrousnetwork
Bone cells in the area die
-
7/31/2019 Fracture Todo Na
25/152
-
7/31/2019 Fracture Todo Na
26/152
-
7/31/2019 Fracture Todo Na
27/152
FRACTURE REPAIR
STEP 4Osteoblasts and osteocytes
continue to remodel thefracture for up to a year.
At this point any cast orexternal support can beremoved
-
7/31/2019 Fracture Todo Na
28/152
-
7/31/2019 Fracture Todo Na
29/152
6 Stages of Fracture Healing
(Bone Repair)
1. Hematoma & inflammation
2. Angiogenesis & cartilage formation
3. Cartilage calcification (Procallus)4. Cartilage removal
5. Bone formation (Callus3 to 4 months
ossification with major adult long bonefracture)
6. Bone remodeling (may take months to years)
-
7/31/2019 Fracture Todo Na
30/152
FACTORS INFLUENCE THEHEALING TIME OF FRACTURES
If realignment is poor, the bone ends may notmeet or there may be soft tissue interposedbetween the bone ends. Union will not occurunder such circumstances.
If the immobilization is inefficient, union may notoccur.
The age and physical condition of the patient, aswell as dietary deficiencies, will affect the healingtime.
-
7/31/2019 Fracture Todo Na
31/152
FACTORS INFLUENCE THE HEALINGTIME OF FRACTURES
Additional factors in healing time are the type of fracture,
its location, and
the adequacy of the blood supply to theaffected area.
Finally, the presence of infection willseverely handicap healing or prevent italtogether.
-
7/31/2019 Fracture Todo Na
32/152
EMERGENCY MANAGEMENT
If fracture is suspected, IMMOBILIZE thebody part immediately after the injurybefore moving the patient
Open fracture are covered with steriledressing to prevent contamination
-
7/31/2019 Fracture Todo Na
33/152
THE OBJECTIVES OF THETREATMENT OF FRACTURES
(1) To regain and maintain the normalalignment of the injured part.
(2) To regain normal function of the injuredpart.
(3) To achieve the above objectives for thepatient in the shortest time possible.
-
7/31/2019 Fracture Todo Na
34/152
PRINCIPLES OF FRACTUREMANAGEMENT
(1)Reduction. Reduction is the process ofrestoring the bone ends (and any fracturedfragments) into their normal anatomical
positions.
- This is accomplished by open or closed
manipulation of the affected area, referred toas open reduction and closed reduction.
-
7/31/2019 Fracture Todo Na
35/152
REDUCTION
(a) Closed reduction is accomplished by bringing thebone ends into alignment by manipulation and manualtraction.
X-rays are taken to determine the position of the bones.
A cast is normally applied to immobilize the extremity andmaintain the reduction.
(b) In open reduction, a surgical opening is made,
allowing the bones to be reduced manually under directvisualization.
Frequently, internal fixation devices will be used to maintain thebone fragments in reduction
-
7/31/2019 Fracture Todo Na
36/152
-
7/31/2019 Fracture Todo Na
37/152
PRINCIPLES OF FRACTUREMANAGEMENT
(2) Immobilization. Immobilization is necessary tomaintain fracture reduction until healing occurs.Immobilization may be accomplished by externalor internal fixation.
(a) Methods of external fixation include casts, splints,and continuous traction.
(b) Internal fixation devices include pins, wires,screws, rods, nails, and plates. These devices,attached to the sides of the bone or inserted throughthe bone, provide internal immobilization of the bone.
-
7/31/2019 Fracture Todo Na
38/152
PRINCIPLES OF FRACTUREMANAGEMENT
(3) Rehabilitation. Rehabilitation is the regainingof strength and normal function in the affectedarea.
Specific rehabilitation for each patient will be basedupon the type of fracture and the methods ofreduction and immobilization used.
The physician will generally consult with the physical
therapist to develop an individualized rehabilitationplan for each patient.
This plan is normally implemented and controlled bythe physical therapy department.
-
7/31/2019 Fracture Todo Na
39/152
NURSING MANAGEMENT OF APATIENT WITH A FRACTURE
a. Nursing care of a patient with a fracture,whether casted or in traction, is basedupon prevention of complications while
healing.
b. By performing an accurate nursingassessment on a regular basis, the nursing
staff can manage the patient's pain andprevent complications.
h h
-
7/31/2019 Fracture Todo Na
40/152
When assessing a patient with afracture, check the "5 P's"
(1)Pain. Worsening pain may indicate increased edema,lack of adequate blood supply, or tissue damage.
(2) Pulse. Check the peripheral pulses, especially those
distal to the fracture site.
(3) Pallor. Observe the color and temperature of the skin,especially around the fracture site.
(4) Paresthesia. Examine the injured area for increase ordecrease in sensation.
(5) Paralysis. Check the patient's mobility.
-
7/31/2019 Fracture Todo Na
41/152
In addition to the five P's mentioned above, the patient'slevel of consciousness and temperature should bechecked regularly.
Mental status changes and temperature elevation could indicatethe presence of infection.
Reposition the patient as necessary to relieve pressureareas.
Check all dressings, bandages, casts, splints, andtraction equipment to ensure that nothing is causingconstriction or pressure.
Frequent and thorough checking and observation on thepart of the nursing staff will promote healing andprevent complications.
-
7/31/2019 Fracture Todo Na
42/152
LIFE THREATENING COMPLICATIONS
Deep venous thrombosis (DVT)
Anterior tibial or femoral veins
May be caused by immobility
Findings include calf pain, positive Homan'ssign
Immediately after operations
anticoagulant therapy antiemboli stockings (usually)
sequential compression device (possibly)
-
7/31/2019 Fracture Todo Na
43/152
-
7/31/2019 Fracture Todo Na
44/152
Pulmonary embolism (PE)
Findings include chest pain (pleuritic), suddenshortness of breath, tachycardia, palpitations,or change in mental status
If PE is suspected,do not leave client. Getcharge nurse to notify health care providerimmediately
Diagnosis confirmed via ventilation/perfusionscan or pulmonary angiography
Continuous IV heparin therapy usuallyprescribed
-
7/31/2019 Fracture Todo Na
45/152
Fat embolism
Definition: fat cells enter pulmonarycirculation
Associated with
multiple trauma accidents
multiple organ involvement
fractures of marrow producing bones
joint replacements
insertion of intermedullary rods Usually occurs 24 to 48 hours after the
fracture
-
7/31/2019 Fracture Todo Na
46/152
Hemorrhage
Abnormal loss of blood from thebody
Most common in fractures ofbone marrow producing bones
-
7/31/2019 Fracture Todo Na
47/152
Gas Gangrene
Gas gangrene is a severe infection of skeletalmuscle caused by the bacteria Clostridium.
These bacteria are anaerobes and spore
formers normally found in soil and in theintestinal tract of man.Gas gangrene occurs most often in wounds
that have been grossly contaminated at the
time of injury, in wounds that have a smallbut deep open wound area, and in woundsthat have a compromised blood supply andtherefore a decreased oxygen supply.
-
7/31/2019 Fracture Todo Na
48/152
Gas Gangrene
Nursing personnel should observe for signs ofapprehension, fever, chills, increased pulse,increased respiratory rate, and frothy foul-smelling
drainage from the wound. In treating gas gangrene, the physician will open
the wound for debridement and irrigation.
Antibiotic therapy and hyperbaric oxygen therapy
will be initiated. Frequently, amputation of theaffected extremity is necessary.
-
7/31/2019 Fracture Todo Na
49/152
Tetanus.
Tetanus is an acute infection caused by thetetanus bacillus, another anaerobic sporeformer.
The bacteria is introduced through a woundthat has been contaminated with soil, feces,or dust.
Toxins that have an affinity for nervoustissue cause hyperirritability, restlessness,muscle rigidity, and tonic muscular spasmsof almost every muscle group.
-
7/31/2019 Fracture Todo Na
50/152
TETANUS
The patient may have difficulty opening themouth due to spasm of facial muscles.Tetanus is sometimes referred to as
"lockjaw" for this reason.Treatment is similar in nature to that of
gangrene, with the addition of anti-
convulsive drugs.
-
7/31/2019 Fracture Todo Na
51/152
CASTSA rigid, external immobilizing device
Uses:
Immobilize a reduced fracture
Correct a deformity
Apply uniform pressure to underlying softtissues
Provide support and to stabilize a weakenedjoint
-
7/31/2019 Fracture Todo Na
52/152
Types of cast
Short-arm cast extends from below theelbow to the palmar crease, secured aroundthe base of the thumb. If thethumb isincluded, it is known as theThumb-spicaor gauntlet cast.
Long-arm cast Extends from the axillaryfold to the proximal palmar crease. Theelbow is usually immobilized at a rightangle.
-
7/31/2019 Fracture Todo Na
53/152
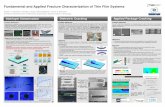
Long-Arm and Short-Leg Cast andCommon Pressure Areas
-
7/31/2019 Fracture Todo Na
54/152
Types of cast
Short-leg cast
Extends from below theknee to the base of the toes. The foot isflexed at a right angle in a flexed position
Long-leg cast Extends from the junction upperand middle third of the thigh to the base of thetoes. The knees may be slightly flexed.
Walking cast A short- or long- leg castreinforced for strength.
-
7/31/2019 Fracture Todo Na
55/152
Types of cast
Body cast Encircles the trunk
Shoulder spica cast A body jacket that
encloses the trunk and the shoulder andelbow
Hip spica cast Encloses the trunk and alower extremity. Adouble hip spicacastincludes both legs
-
7/31/2019 Fracture Todo Na
56/152
Casting Materials:
Nonplaster (Fiberglass)
Water activated polyurethane material havingthe versatility of plaster cast but is lighter in
weight, stronger, water resistant and durable.
Used for non displaced fractures with minimal
swelling and for long-term wear
-
7/31/2019 Fracture Todo Na
57/152
Nonplaster (Fiberglass)
Characteristic of non plaster cast (Fiberglass):
Consist of an open-weave, non absorbent fabricimpregnated with cool water-activated hardeners
Bond and reach full rigid strength in minutes
Porous and therefore diminish skin problems
Do not soften when wet, which allows forhydrotherapy
When wet, they are dried with a hair dyer on a coolsetting (thorough drying is important to preventskin breakdown)
-
7/31/2019 Fracture Todo Na
58/152
Casting Materials:
Plaster Traditional cast Rolls of plaster bandage are wet in cool water and
applied smoothly to the body.
A crystallizing reaction occurs and heat is given off (anexothermic reaction).
The heat given off during this reaction can beuncomfortable to the client, and the nurse shouldinform the patient about the sensation of increasing
warmth Cast needs to be exposed to air (i.e., uncovered) to
allow maximum dissipation of heat; most casts coolafter about 15min
-
7/31/2019 Fracture Todo Na
59/152
Plaster
After the plaster sets, the cast remains wetand somewhat soft; it does not have its fullstrength until it is dry.
While the cast is DAMP, it can be dented. It must be handled by palms of the hands
Not allowed to rest on hard surfaces or sharpedges
Cast dents may press on the skin, causingirritation and skin breakdown.
-
7/31/2019 Fracture Todo Na
60/152
Plaster
Characteristics of plaster cast:
Plaster cast requires 24 to 72 hours to drycompletely
Awet plaster cast appears DULL andGRAY, sounds dull on percussion, feels dampand smells musty.
Adry plaster cast is WHITE and SHINY,resonant to percussion, odorless and firm.
-
7/31/2019 Fracture Todo Na
61/152
HEALTH TEACHINGS
Prior to cast application
Explain condition necessitating the
castExplain purpose and goals of the cast
Describe expectations during the
casting process: e.g., the heat fromhardening plaster
CARE OF THE PATIENT WITH A
-
7/31/2019 Fracture Todo Na
62/152
CARE OF THE PATIENT WITH ANEWLY APPLIED CAST
a. Expose a newly applied cast to aircirculation.
It should never be covered,
b. Handle a wet cast carefully.
Never use fingers as they will leave
indentations, which cause pressure areas withinthe cast.
CARE OF THE PATIENT WITH A
-
7/31/2019 Fracture Todo Na
63/152
CARE OF THE PATIENT WITH ANEWLY APPLIED CAST
c. Provide plastic-covered pillows to support the castalong its entire length. Never permit the wet cast to rest directly on a flat or
firm surface
d. Review the patient's clinical record for the type ofcast and the reason the cast has been applied. Determine PT.s knowledge of the cast purpose and
whether he has had a cast before. Instruct the patient on care of the cast that is wet and
after it is dry.
CARE OF THE PATIENT WITH
-
7/31/2019 Fracture Todo Na
64/152
CARE OF THE PATIENT WITHA NEWLY APPLIED CAST
e. After a cast has cooled and begins toharden, elevate the casted extremity toreduce swelling which often occurs after
application of a cast. For example, hand higher than elbow, elbow
higher than shoulder.
f. Observe all edges of the cast for anyareas that cut or put pressure on the skin.
CARE OF THE PATIENT WITH A
-
7/31/2019 Fracture Todo Na
65/152
CARE OF THE PATIENT WITH ANEWLY APPLIED CAST
Observe the extremity encased in plaster forcirculatory impairment by comparing fingersor toes of the casted extremity with the
uninvolved extremity.
Circulation should be checked hourly during
the first 24 to 48 hours, then every 4 hours.
Assessment of circulation on
-
7/31/2019 Fracture Todo Na
66/152
Assessment of circulation ona casted extremity
(1) Check the skin temperature of the injured extremity. Itshould not be colder than the unaffected limb.
(2) Check and compare the pulses. They should be equal.
(3) Check for complaints of numbness, tingling, burning,swelling, pain, pressure, or inability to move the fingersor toes.
(4) Report presence of the above signs and symptomsIMMEDIATELY to avoid possible tissue necrosis; thesefindings indicate possible ischemia.
Assessment of circulation on
-
7/31/2019 Fracture Todo Na
67/152
Assessment of circulation ona casted extremity
Perform the blanching (capillary refill) test.
(1) "capillary refill, less than 3 seconds
(2) Failure to blanch, or a blue tinge, - indicates
impaired venous circulation and congestionof tissues.
(3) Failure of color to return, or cold, pale fingers or
toes -suggests impaired arterial circulation.(4) In either case, report findings IMMEDIATELY. Do
not wait. Permanent damage can result fromimpaired circulation caused by cast pressure.
-
7/31/2019 Fracture Todo Na
68/152
-
7/31/2019 Fracture Todo Na
69/152
FINISHING THE DRY CAST
c. Nursing implications. A cast without a smooth,unwrinkled finish is a potential source of problems.
(1) Rough, unfinished cast edges will scrape or cut theskin. Broken skin surfaces may become infected.
(2) Loose bits of plaster from an unfinished cast maybecome lodged inside the cast, causing itching andirritation.
(3) Wrinkled or "bunched-up" edging may result inpressure areas and potential skin breakdown.
-
7/31/2019 Fracture Todo Na
70/152
COMPLICATIONS
Compartment syndrome Occurs when there is an increased pressure within a
limited space (e.g., cast, muscle compartment) thatcompromises the circulation and function of the tissue
within the confined area. To relieve the pressure the cast must be bivalved (cut in
half longitudinally) while maintaining alignment, and theextremity must be elevated no higher than heart level toensure arterial perfusion
If pressure is not restored, a fasciotomy may benecessary to relieved the pressure within the musclecompartment.
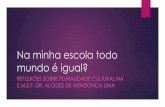
Cross Section of Normal Muscle
-
7/31/2019 Fracture Todo Na
71/152
Compartments and Cross Section WithCompartment Syndrome
-
7/31/2019 Fracture Todo Na
72/152
CAST CUTTING
Casts may be cut for different reasons to allow for wound dressings,
to examine a painful area, or
to relieve pressure.
Nursing personnel may be required to assist
with cast cutting at the bedside as anemergency measure.
C S C G
-
7/31/2019 Fracture Todo Na
73/152
CAST CUTTING
a. Bivalving the Cast. Bivalving is the recommended method for
emergency cutting to relieve pressure.
In bivalving, the cast must be cut along itsentire length on two sides (medial and lateral)and the base lining or padding cut completelydown to the skin.
To cut the cast, use a knife, a hand cutter, or anelectric cast cutter.
Use bandage scissors to cut the base material. Touse a knife for emergency cast cutting, follow thesesteps.
-
7/31/2019 Fracture Todo Na
74/152
FAILURE OF UNION
-
7/31/2019 Fracture Todo Na
75/152
FAILURE OF UNION
malunion fracture healing is not stopped but slowed
prevention of malunion
reduce and immobilize properly be sure client understands limits on activity and position
delayed union
fracture does not heal
more common with multiple fracture fragments
no evidence of fracture healing four to six months afterthe fracture
GENERAL NURSINGMANAGEMENT OF THE PATIENT
-
7/31/2019 Fracture Todo Na
76/152
MANAGEMENT OF THE PATIENTWITH A CAST
(1) Check the edges of the cast and all skinareas where the cast edges may causepressure.
If there are signs of edema or circulatoryimpairment, notify the charge nurse orphysician immediately.
(2) Slip your fingers under the cast edges to
detect any plaster crumbs or other foreignmaterial. Move the skin back and forthgently to stimulate circulation.
-
7/31/2019 Fracture Todo Na
77/152
(3) Lean down and smell the cast to detect
odors indicating tissue damage.A musty or moldy odor at the surface of the
cast may be the first indication that necrosisfrom pressure has developed underneath.
(4) Check the integrity of the cast bylooking for cracks, breaks, and soft spots.
A th t d t b h ki th f ll i
-
7/31/2019 Fracture Todo Na
78/152
Assess the casted part by checking the following.
(1) Assess circulation by performing the blanching
test and comparing the skin temperature andblanching reaction of the affected limb to that ofthe unaffected limb.
(2) Assess the presence of sensation in the
affected limb by touching exposed areas of skinand instructing the patient to describe what hefelt.
(3) Assess the motor ability of the affected limb byhaving the patient wiggle his fingers or toes.
P ti t d ti
-
7/31/2019 Fracture Todo Na
79/152
Patient education(1) Avoid resting cast on hard surfaces or sharp
edges that may dent the cast and causepressure areas.
(2) Never use a coat hanger or other foreignobject to "scratch" inside the cast. This may
cause skin damage and infection.(3) Report any danger signs to the nursing staffimmediately. Danger signs include pale, cold fingers or
toes, tingling, numbness, increased pain, pressure
spots, odor, or feeling that the cast has become tootight.
(4) Report any damage to the cast such ascracks, breaks, or soft spots.
(5) Never attempt to remove or alter the cast.
-
7/31/2019 Fracture Todo Na
80/152
E t l Fi ti D i
-
7/31/2019 Fracture Todo Na
81/152
External Fixation Devices
Used to manage open fractureswith soft-tissue damage
Provide support for complicatedor comminuted fractures
Reassure patient concerned byappearance of device
-
7/31/2019 Fracture Todo Na
82/152
E t l Fi ti D i
-
7/31/2019 Fracture Todo Na
83/152
External Fixation Devices
Discomfort is usually minimal, and earlymobility may be anticipated with thesedevices
Elevate to reduce edema
Monitor for signs and symptoms of
complications, including infection
Provide pin care (chlorhexidine solution)
Patient teaching
-
7/31/2019 Fracture Todo Na
84/152
Patient teaching
Report any signs of infection (redness,swelling, purulent drainage, and fever)
Instruct proper pin care at home; cleantechnique can be observed at home
The nurse instructs pt. and family aboutneurovascular checks (Five Ps) and report
any change promptly
Patient teaching
-
7/31/2019 Fracture Todo Na
85/152
Patient teaching
Check the integrity of fixator device, reportany loose pins or clamps immediately
Emphasize the importance of adhering to
weight- bearing instructions to minimizeloosening of the pins
Refer for physical therapy re: ambulationand safe use of ambulatory aids
OPEN REDUCTION AND
-
7/31/2019 Fracture Todo Na
86/152
INTERNAL FIXATION
Open reduction surgical procedures wherethe fracture fragments are realigned
It is usually performed with INTERNALFIXATION where screws, plates, pins,wires or nails mat be used to maintain
alignment of the fractured fragments
-
7/31/2019 Fracture Todo Na
87/152
Traction
-
7/31/2019 Fracture Todo Na
88/152
Traction
The application of pulling force to an injuredbody part or extremity while a countertraction pulls in the opposite direction
The pulling force can be achieved throughthe use of hand (manual traction) or more
commonly the application of weights
All t ti d t b li d i t
-
7/31/2019 Fracture Todo Na
89/152
All traction needs to be applied in twodirections. The lines of pull are vectors of
force. The result of the pulling force isbetween the two lines of the vectors offorce.
Countertraction is supplied by
-
7/31/2019 Fracture Todo Na
90/152
Countertractionis supplied bythepatient's body weight and
friction against the bed.
Additional countertraction maybe achieved by elevating thehead or foot of the bed or by
application of counter tractionapparatus
-
7/31/2019 Fracture Todo Na
91/152
Purposes of Traction
-
7/31/2019 Fracture Todo Na
92/152
Purposes of Traction
Reduce muscle spasms
Reduce, realign, immobilize andpromote healing of fractured bones
Reduce deformity
Increase space between opposingforces
Used as a short-term intervention untilother modalities are possible
Principles of Effective Traction
-
7/31/2019 Fracture Todo Na
93/152
Principles of Effective Traction
Whenever traction is applied, acounterforce must be applied;frequently the patients body weight andpositioning in bed supply the counterforce
Traction must be continuous to reduceand immobilize fractures
Skeletal traction is never interrupted
Principles of Effective Traction
-
7/31/2019 Fracture Todo Na
94/152
Principles of Effective TractionWeights are not removed unless
intermittent traction is prescribed
Any factor that reduces pull must be
eliminated
Ropes must be unobstructed and weightsmust hang freely
Knots or the footplate must not touch thefoot of the bed
Types of Traction
-
7/31/2019 Fracture Todo Na
95/152
Types of Traction
Skin traction Light traction delivered to a bone bypulling on adhesive strips attached to
the skin of an extremity;
Capable of delivering a traction forceof approximately 10lb
Skin traction
-
7/31/2019 Fracture Todo Na
96/152
Skin traction
Used frequently for the reduction offractures in young children
Common example of skin traction:Bucks extension traction
Cervical head halter ( to treat neck
pain)Pelvic traction (sometimes used totreat back pain)
Prior to application of the skin
-
7/31/2019 Fracture Todo Na
97/152
Prior to application of the skintraction,
inspect the skin for rashes,abrasions, or signs of circulatory
impairmentthe skin must be healthy inorder to tolerate the traction.
Check with the physician as to whetherthe skin should be shaved
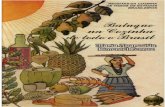
BUCKS EXTENSION TRACTION
-
7/31/2019 Fracture Todo Na
98/152
BUCKS EXTENSION TRACTIONThis form of skin traction to the lower limb
provides for straight pull through a single pulleyattached to a crossbar at the foot of the bed.
The limb in traction lies parallel to the bed.
The foot of the bed is routinely elevated to providecounter traction and to keep the patient frombeing pulled down to the foot of the bed.
In Buck's extension traction, the patient isusuallynot allowed to turn and must remainflat on his back.
-
7/31/2019 Fracture Todo Na
99/152
-
7/31/2019 Fracture Todo Na
100/152
RUSSELL TRACTION
-
7/31/2019 Fracture Todo Na
101/152
RUSSELL TRACTION
In this form of skin traction, a system of suspension andtraction pull is used.
Adhesive strips are applied as in Buck's extension, and theknee is suspended in a sling. A rope is attached to the
sling's spreader bar.
This rope There is an upward pull from the sling pulley anda forward pull from the pulleys at the foot of the bed.
In Russell traction, the angle between the thigh andthe bed is approximately 20 and there is always slightflexion of both the hip and the knee.
PELVIC TRACTION GIRDLE
-
7/31/2019 Fracture Todo Na
102/152
PELVIC TRACTION GIRDLE
ordinarily used for treatment of low back pain andmuscle spasm.
It is fitted snugly and evenly over the iliac crests.
The traction straps, extending on the lateral sideof each thigh, are hooked to a separate rope atmid-thigh level and each rope leads to a separatebut equal weight at the foot of the bed.
The foot of the bed is usually elevated to providecounter traction.
CERVICAL TRACTION HALTER
-
7/31/2019 Fracture Todo Na
103/152
CERVICAL TRACTION HALTER
A canvas head halter is used for treatment ofaffections of the cervical spine. The halter fitssnugly under the chin and around the back of thehead against the occipital protuberance.
A pulley rope is attached to the spreader bar thathooks to the top of the harness. The prescribedweights at the end of the pulley rope keep the
patient's neck and cervical spine in a positionspecified by the physician.
-
7/31/2019 Fracture Todo Na
104/152
-
7/31/2019 Fracture Todo Na
105/152
CERVICAL TRACTION
-
7/31/2019 Fracture Todo Na
106/152
CERVICAL TRACTIONCrutchfield or Vinke tongs are used for
skeletal traction in the treatment offractures of the cervical spine.
The tong points are inserted in the parietal
area of the skull (just in the outer layers ofthe bone) and the tong is then attached tothe pulling device.
The procedures may be done under localanesthesia in the operating room or on theward.
-
7/31/2019 Fracture Todo Na
107/152
-
7/31/2019 Fracture Todo Na
108/152
The Thomas splint (half ring) is applied ini ith th i fitt d t i l
-
7/31/2019 Fracture Todo Na
109/152
various ways: with the ring fitted posteriorlyagainst the ischium or anteriorly in the groin. The
thigh rests in a canvas or bandage-strip sling withthe popliteal space left free.
The Pearson attachment is attached by clamps to
the Thomas splint at knee level. A canvas orbandage-strip sling supports the lower leg andprovides the desired degree of knee flexion.
Afootplate is attached to the distal end of thePearson attachment to support the foot in aneutral position. The heel should be left free.
-
7/31/2019 Fracture Todo Na
110/152
ARM TRACTION
-
7/31/2019 Fracture Todo Na
111/152
ARM TRACTIONThe type of traction used for the upper
extremities will depend upon the locationof the fracture, any associated injuries, andthe preference of the physician.
As with other body parts, the arm may beimmobilized in skin traction or skeletaltraction.
The position of the arm in traction may besidearm or overhead.
-
7/31/2019 Fracture Todo Na
112/152
Preventive Interventions
-
7/31/2019 Fracture Todo Na
113/152
Preventive Interventions
Promptly report any alteration insensation or circulation
Provide frequent back care andskin care
Regularly shift position
Special mattresses or otherpressure-reduction devices
Preventive Interventions
-
7/31/2019 Fracture Todo Na
114/152
Preventive Interventions
Perform active foot and leg exercises everyhour
Elastic hose, pneumatic compression hose,
or anticoagulant therapy may be prescribedTrapeze to help with movement for patients
in skeletal traction
Pin care
Exercises to maintain muscle tone andstrength
Nursing ProcessAssessmentf th P ti t i T ti
-
7/31/2019 Fracture Todo Na
115/152
of the Patient in Traction
Assessneurovascular statusand forcomplications
Assess formobility-relatedcomplicationsof pneumonia, atelectasis,constipation, nutritional problems, urinary
stasis, and UTI
Assess forpain and discomfort
Nursing ProcessAssessmentf th P ti t i T ti
-
7/31/2019 Fracture Todo Na
116/152
of the Patient in Traction
Assess emotional and behavioralresponses
Assess coping ability
Assess thought processes
Assess knowledge
NURSING MANAGEMENT OF THEPATIENT IN TRACTION
-
7/31/2019 Fracture Todo Na
117/152
PATIENT IN TRACTION
Prevent skin breakdown, nerve pressure,and circulatory impairment
Measures to reduce anxiety Provide and reinforce information
Encourage patient participation in decisionmaking and in care
Encourage frequent visits (family andcaregivers/ nurse) to reduce isolation
Provide diversional activities
NURSING MANAGEMENT OF THEPATIENT IN TRACTION
-
7/31/2019 Fracture Todo Na
118/152
PATIENT IN TRACTION
Use assistive devices Arrange consultation with/referral for physical therapy
Prevention of atelectasis and pneumonia Auscultate lungs every 4 to 8 hours Encourage coughing and deep breathing exercises
High-fiber diet Encourage fluids
Identify and include food preferences and encourageproper diet
THE ORTHOPEDIC BED
-
7/31/2019 Fracture Todo Na
119/152
THE ORTHOPEDIC BED
-
7/31/2019 Fracture Todo Na
120/152
-
7/31/2019 Fracture Todo Na
121/152
-
7/31/2019 Fracture Todo Na
122/152
-
7/31/2019 Fracture Todo Na
123/152
WHEELCHAIRS The folding wheelchair is the most commonly used
mobilization device for a patient who can sit upright.
If leg elevation is required, a special board or legattachment can be secured to the chair and pillow orcushion support provided.
The use of a wheelchair allows the patient to be out ofbed, mobile, and moderately independent.
-
7/31/2019 Fracture Todo Na
124/152
WHEELCHAIR
-
7/31/2019 Fracture Todo Na
125/152
-
7/31/2019 Fracture Todo Na
126/152
-
7/31/2019 Fracture Todo Na
127/152
-
7/31/2019 Fracture Todo Na
128/152
CRUTCHES
Crutches are used to promote ambulation andindependence in patients with affected lowerextremities.
The use of crutches is a complicated procedurethat is routinely taught by the physical therapydepartment. There are occasions, however,
when the nursing staff will have thisresponsibility.
CRUTCHES
-
7/31/2019 Fracture Todo Na
129/152
The physician will prescribe the use of crutchesand the gait (crutch-walking method) to beused.
The prescribed gait depends upon the amountof weight bearing permitted on the affectedleg(s).
The crutches must be "fitted" to the patientand instructions given for the prescribed crutch-walking method.
PREPARATION
-
7/31/2019 Fracture Todo Na
130/152
Have the patient lie supine, arms at sides, wearing
a shoe on the unaffected foot.
Using a tape measure, measure from the axilla to
the heel of the shoe and add two inches. Adjustthe crutch shaft to this measurement. Or . . .
Place the crutch along the patient's unaffected
side with the axillary pad at the axilla and thecrutch tip 6 to 8 inches to the side of the heel.
Adjust the crutch to fit this length.
Have the patient stand at the bedside with thecrutches in place and grip the hand bars You
-
7/31/2019 Fracture Todo Na
131/152
crutches in place and grip the hand bars. Youshould be able to fit two fingers between the axilla
and the axillary bar when the patient is standing inthe tripod position
Adjust the hand bar so that the
-
7/31/2019 Fracture Todo Na
132/152
Adjust the hand bar so that thepatient's elbow is flexed approximately30 when the hand grips the hand bar
Check each crutch for proper fit andask the patient if the crutch feelscomfortable.
CRUTCH WALKING GAITS
-
7/31/2019 Fracture Todo Na
133/152
The 4-point gait is used when the patientcan bear some weight on both lowerextremities. Place the patient in the tripodposition and instruct him to do the
following.(1) Move the right crutch forward.
(2) Move the left foot forward.
(3) Move the left crutch forward.
(4) Move the right foot forward.
(5) Repeat this sequence of crutch-foot-crutch-foot for desired ambulation.
-
7/31/2019 Fracture Todo Na
134/152
CRUTCH WALKING GAITS
-
7/31/2019 Fracture Todo Na
135/152
The 3-point gait is used when thepatient should not bear any weight on theaffected leg. Place the patient in the tripodposition and instruct him to do the
following.(1) Move the affected (non-weight bearing) leg
and both crutches forward together.
(2) Move the unaffected (weight bearing) legforward.
(3) Repeat this sequence for desired ambulation.
-
7/31/2019 Fracture Todo Na
136/152
CRUTCH WALKING GAITS
-
7/31/2019 Fracture Todo Na
137/152
The 2-point gait is used when thepatient can bear some weight on both lowerextremities. Place the patient in the tripodposition and instruct him to do the
following.(1) Move the right leg and left crutch forward
together.
(2) Move the left leg and the right crutch forwardtogether.
(3) Repeat this sequence for desired ambulation.
-
7/31/2019 Fracture Todo Na
138/152
CRUTCH WALKING GAITS
-
7/31/2019 Fracture Todo Na
139/152
Swing-through gait is used forpatients with lower extremities that areparalyzed and/or in braces. Place thepatient in the tripod position and instruct
him to do the following:(1) Move both crutches forward together about 6
inches.
(2) Move both legs forward together about 6inches.
(3) Repeat the sequence in rhythm for desiredambulation
-
7/31/2019 Fracture Todo Na
140/152
-
7/31/2019 Fracture Todo Na
141/152
WALKERS AND CANES
-
7/31/2019 Fracture Todo Na
142/152
Walkers and canesare generally used as mobilizationaids for patients who can bear weight on the affected leg,but require some support.
When utilizing a walker, the patient should use themuscles of the arms and upper body to help support hisweight. After placing the walker in front of the patient,instruct the patient to ambulate with a walker using thefollowing sequence of moves.
(1) Firmly grasp the hand grips.(2) Move the walker and the affected leg forward about 6 inches.
(3) Move the unaffected leg forward, parallel to the affected leg.
(4) Repeat the sequence for each step.
-
7/31/2019 Fracture Todo Na
143/152
WALKERS AND CANES
-
7/31/2019 Fracture Todo Na
144/152
When utilizing a cane, the patientshould hold a cane on the unaffected sidewith his elbow slightly flexed and the canetip about 6 inches in front of and 6 inches to
the side of his foot. (A cane is used for balance, rather than physical
support. It is held on the unaffected side to
prevent the patient from "leaning" on it forsupport.)
CANE
-
7/31/2019 Fracture Todo Na
145/152
Instruct the patient to ambulate with a cane using
the following sequence.(1) Move the affected leg forward, parallel to the cane.
(2) Move the unaffected leg forward so that the heel isjust beyond the cane.
(3) Move the affected leg forward so that it is even withthe unaffected leg.
(4) Move the cane forward 6 inches to the front and 6inches to the side of the patient (starting position).
(5) Repeat the sequence for desired ambulation. If lesssupport is needed, the cane and the affected leg can bemoved together.
-
7/31/2019 Fracture Todo Na
146/152
-
7/31/2019 Fracture Todo Na
147/152
OtherMusculoskeletal trauma
Contusion
-
7/31/2019 Fracture Todo Na
148/152
Injury to the soft tissue
Causes:
Blunt force
Blow Kick or
Fall
S/Sx Ecchymosis, pain swelling
Contusion: Management
-
7/31/2019 Fracture Todo Na
149/152
Relieve edema and swellingElevate feet (extremity)
Cold compressmax. of 20minsApply pressure bandage
Apply warm compress
After six hours of injury to promoteabsorption
Sprain and Strain
-
7/31/2019 Fracture Todo Na
150/152
Sprain Injury to ligamentous structuresurrounding a joint
Usually caused by wrenching ortwisting
Strain
Injury to muscles or tendons
Caused by twists pull and/or tear
-
7/31/2019 Fracture Todo Na
151/152
Sprain and Strain: Management
-
7/31/2019 Fracture Todo Na
152/152
Teach the importance of stretching andwarming up exercise before strenuousactivity Elastic bandage may also be applied prior to
activity for additional support
Encourage to adhere to exercise program toregain muscle tone and strength
This is in collaboration with the physicaltherapist