FAME 2 anos
25
Apresentação: R2 Hemodinâmica Cristina Silveira
-
Upload
cristina-silveira -
Category
Health & Medicine
-
view
58 -
download
0
Transcript of FAME 2 anos
Apresentação: R2 Hemodinâmica Cristina Silveira

• FFR – Índice de significância fisiológica da estenose coronariana.
• Definido como o fluxo máximo em artéria estenótica, medido durante o cateterismo, em relação ao máximo fluxo normal (Pd/Pa).
FFR – Funcional Flow Reserve (Reserva fracionada de fluxo)
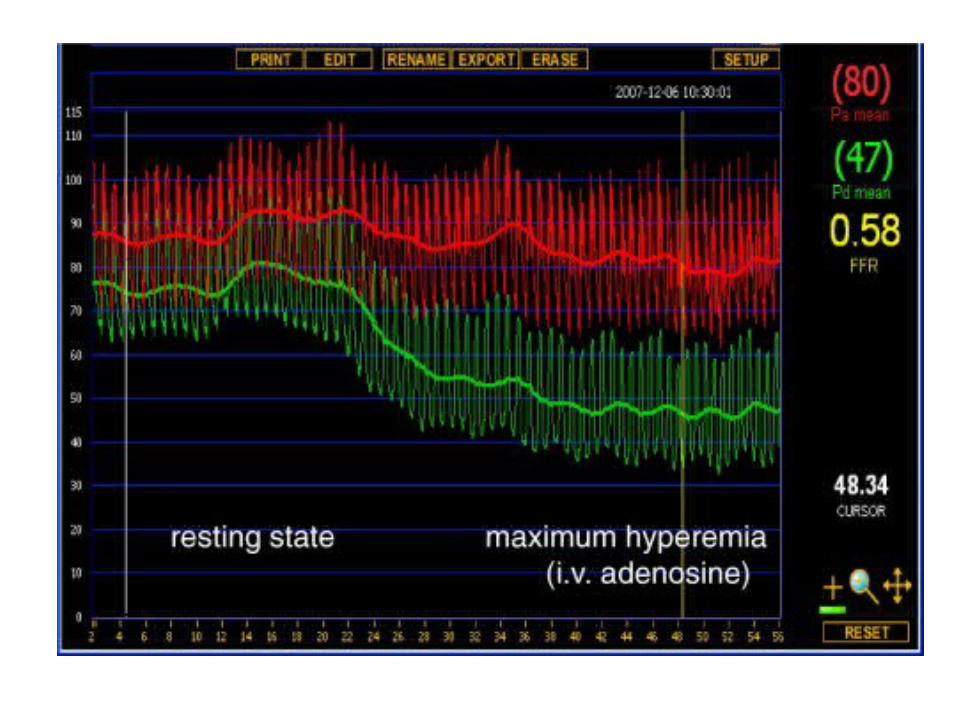
• Medida da pressão coronariana distal à lesão, com o uso de catéter, em relação à pressão aórtica simultaneamente durante hiperemia máxima.
FLUXO SANGÜÍNEO MÁXIMO PROPORCIONADO POR UMA ARTÉRIA ESTENÓTICA COMO FRAÇÃO DO SEU FLUXO MÁXIMO NORMAL
Background
• Em pacientes com DAC estável, ACTP não tem claro benefício no prognóstico • Na prática clínica diária, apenas metade dos pacientes submetidos a ACTP realizou avaliação funcional não invasiva antes do procedimento
• Testes não invasivos tem limitações especialmente em DAC multiarterial
Objetivo
• Comparar desfechos clínicos em pacientes
submetidos a angioplastia guiada por FFR +
tratamento clínico versus tratamento clínico
isolado em pacientes com DAC estável
Critérios de Inclusão
Pacientes encaminhados para ACTP
• Angina estável (CCS 1, 2, 3 ou 4)• Dor atípica ou sem dor porém com isquemia
miocárdica documentada
E
Angiografia com doença de 1, 2, ou 3 vasos
Critérios de Exclusão
1. CRM prévia
2. FE < 30%
3. Lesão TCE
Desfecho primário
Composto de
• Morte por qualquer causa
• Infarto do miocárdio
• Hospitalização não-planejada com revascularização urgente
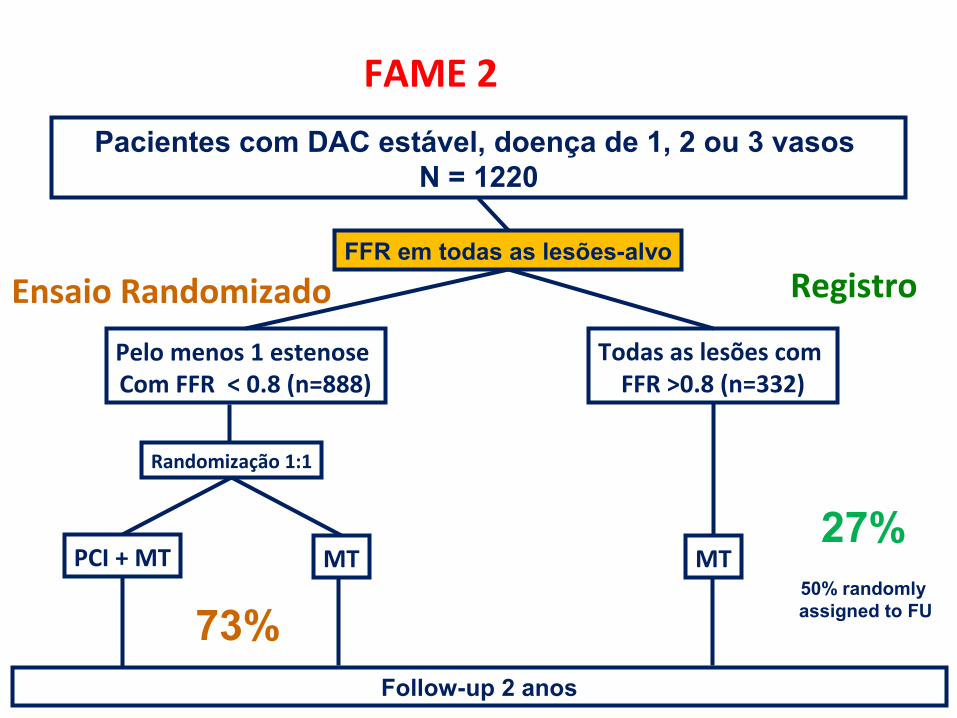
FAME 2
Pacientes com DAC estável, doença de 1, 2 ou 3 vasos N = 1220
FFR em todas as lesões-alvo
Todas as lesões com FFR >0.8 (n=332)
MT
Pelo menos 1 estenose Com FFR < 0.8 (n=888)
Randomização 1:1
PCI + MT MT
Follow-up 2 anos
Registro
50% randomly assigned to FU
27%
Ensaio Randomizado
73%
O Comitê Independente de Segurança recomendou interrupção precoce do estud em Janeiro de 2012 após inclusão de 1220 pacientes (± 54% do número inicialmente planejado)
11
Recomendação DSMB
*DSMB: Stephan Windecker, Chairman, Stuart Pocock, Bernard Gersh
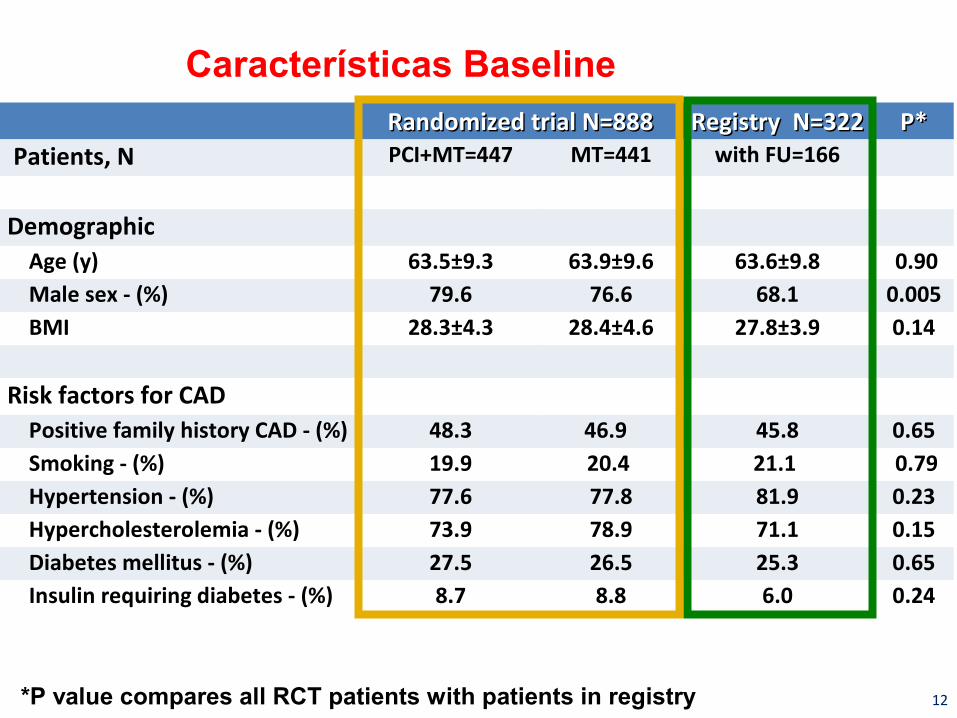
Características Baseline Randomized trial N=888Randomized trial N=888 Registry N=322Registry N=322 P*P* Patients, N PCI+MT=447 MT=441 with FU=166
Demographic Age (y) 63.5±9.3 63.9±9.6 63.6±9.8 0.90 Male sex - (%) 79.6 76.6 68.1 0.005 BMI 28.3±4.3 28.4±4.6 27.8±3.9 0.14
Risk factors for CAD
Positive family history CAD - (%) 48.3 46.9 45.8 0.65 Smoking - (%) 19.9 20.4 21.1 0.79 Hypertension - (%) 77.6 77.8 81.9 0.23 Hypercholesterolemia - (%) 73.9 78.9 71.1 0.15 Diabetes mellitus - (%) 27.5 26.5 25.3 0.65 Insulin requiring diabetes - (%) 8.7 8.8 6.0 0.24
12*P value compares all RCT patients with patients in registry

Características Baseline Randomized trial N=888Randomized trial N=888 Registry N=322Registry N=322 P*P* Patients, N PCI+MT=447 MT=441 with FU=166
Non-Cardiac Co-Morbidity Renal Failure (Cr > 2.0 mg/dL) - (%) 1.8 2.7 4.2 0.14 History of stroke or TIA - (%) 7.4 6.3 6.0 0.69 Peripheral vascular disease - (%) 9.6 10.7 4.8 0.03Cardiac History History of MI - (%) 37.2 37.8 36.6 0.83 History of PCI in target vessel -(%)
17.9 17.2 20.5 0.37
Angina - (%) 0.64 Asymptomatic 11.9 10.5 10.2 CCS class I 18.3 22.3 25.3 CCS class II 45.6 44.8 44.6 CCS class III 17.9 14.8 13.9 CCS class IV, stabilized 6.3 7.7 6.0Silent ischemia- (%) 16.3 16.6 16.3 0.96LVEF < 50% - (%) 19.6 13.7 18.0 0.6913*P value compares all RCT patients with patients in registry
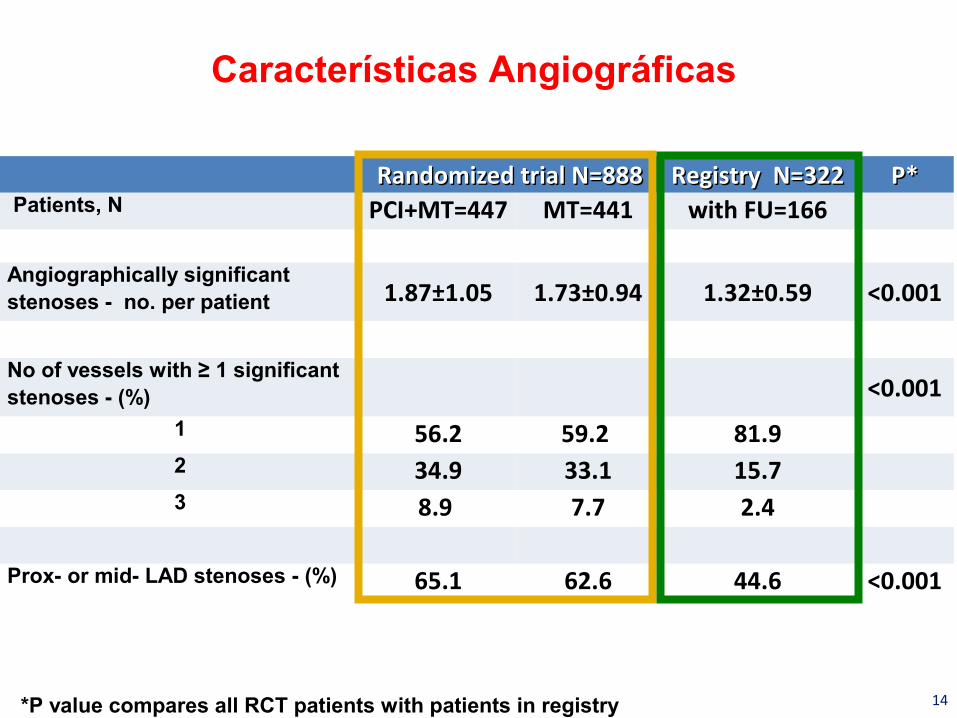
Características Angiográficas
Randomized trial N=888Randomized trial N=888 Registry N=322Registry N=322 P*P* Patients, N PCI+MT=447 MT=441 with FU=166
Angiographically significant stenoses - no. per patient 1.87±1.05 1.73±0.94 1.32±0.59 <0.001
No of vessels with ≥ 1 significant stenoses - (%) <0.001
1 56.2 59.2 81.92 34.9 33.1 15.73 8.9 7.7 2.4
Prox- or mid- LAD stenoses - (%) 65.1 62.6 44.6 <0.001
14*P value compares all RCT patients with patients in registry
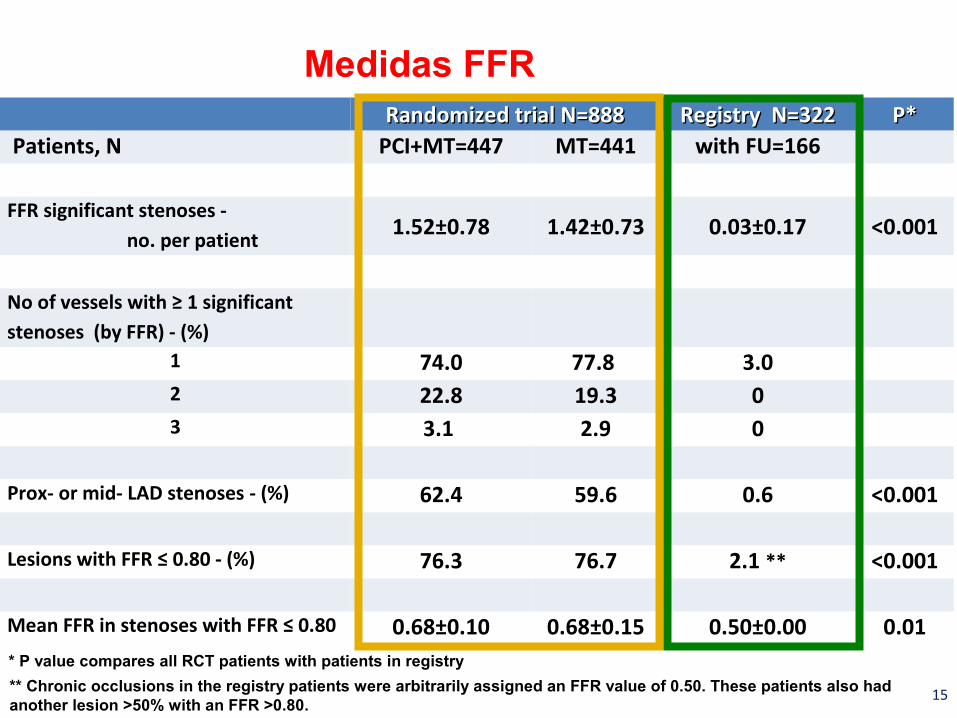
Medidas FFR Randomized trial N=888Randomized trial N=888 Registry N=322Registry N=322 P*P* Patients, N PCI+MT=447 MT=441 with FU=166
FFR significant stenoses - no. per patient
1.52±0.78 1.42±0.73 0.03±0.17 <0.001
No of vessels with ≥ 1 significant stenoses (by FFR) - (%)
1 74.0 77.8 3.02 22.8 19.3 03 3.1 2.9 0
Prox- or mid- LAD stenoses - (%) 62.4 59.6 0.6 <0.001
Lesions with FFR ≤ 0.80 - (%) 76.3 76.7 2.1 ** <0.001
Mean FFR in stenoses with FFR ≤ 0.80 0.68±0.10 0.68±0.15 0.50±0.00 0.01
15
* P value compares all RCT patients with patients in registry
** Chronic occlusions in the registry patients were arbitrarily assigned an FFR value of 0.50. These patients also had another lesion >50% with an FFR >0.80.
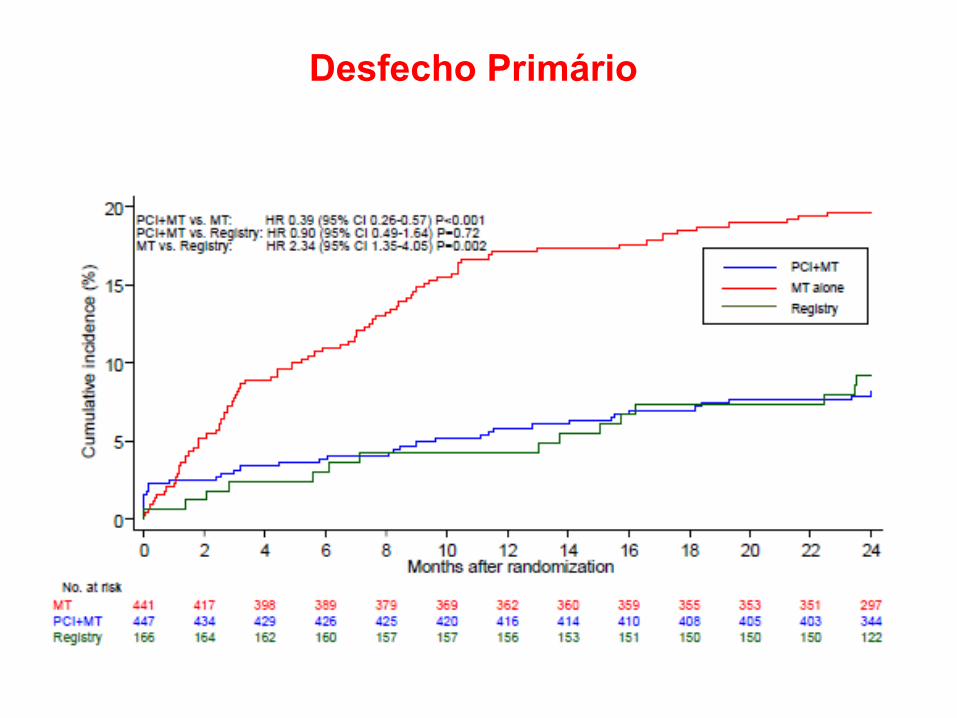
Desfecho Primário
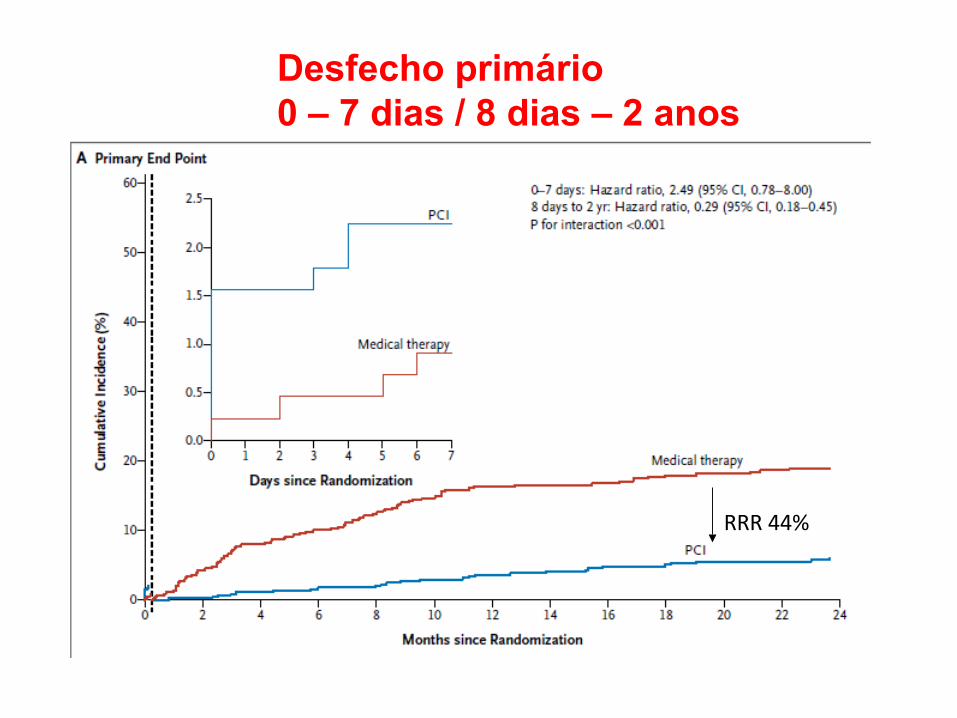
Desfecho primário0 – 7 dias / 8 dias – 2 anos
RRR 44%
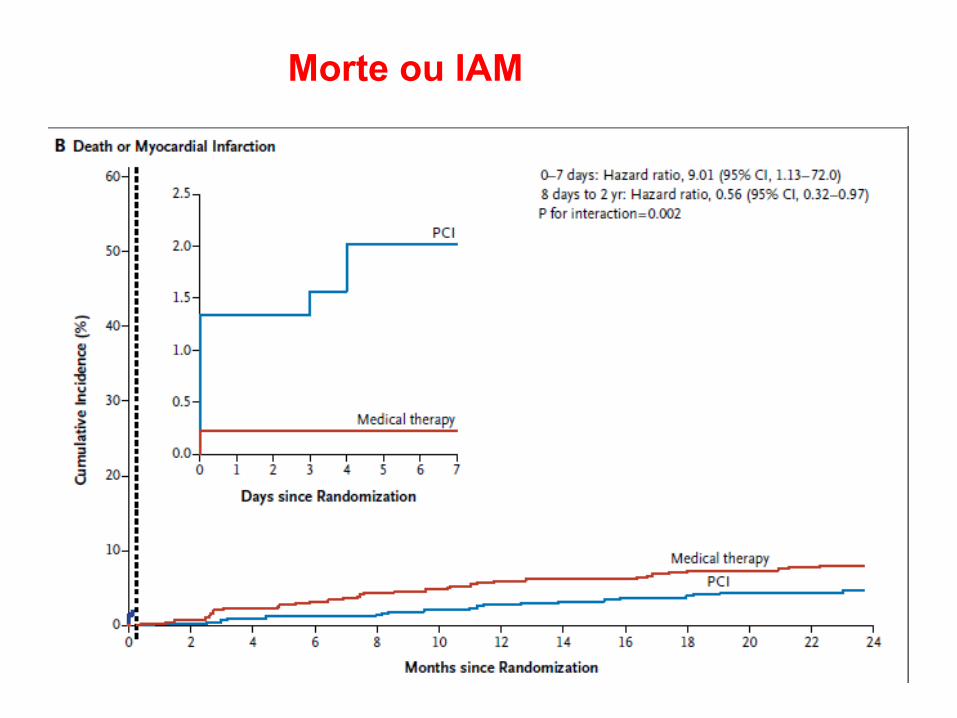
Morte ou IAM
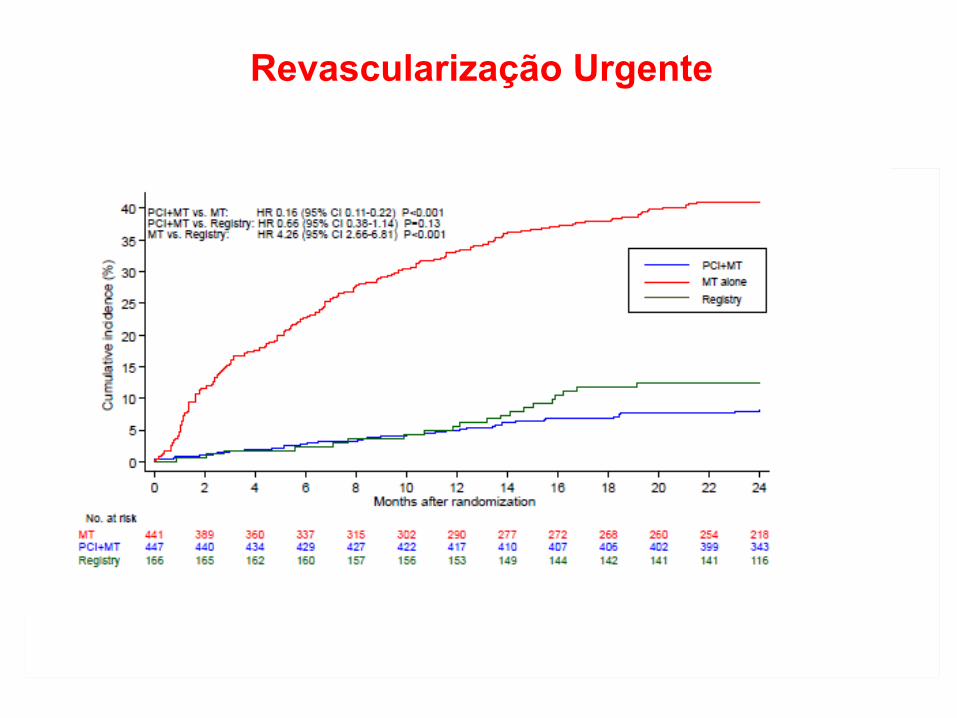
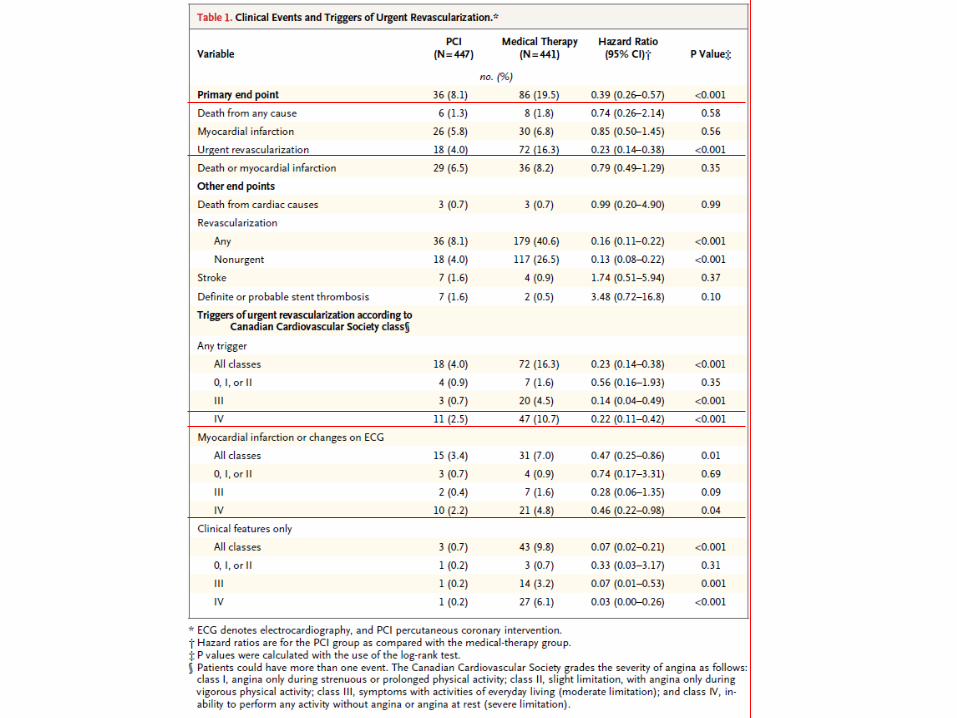
Revascularização Urgente
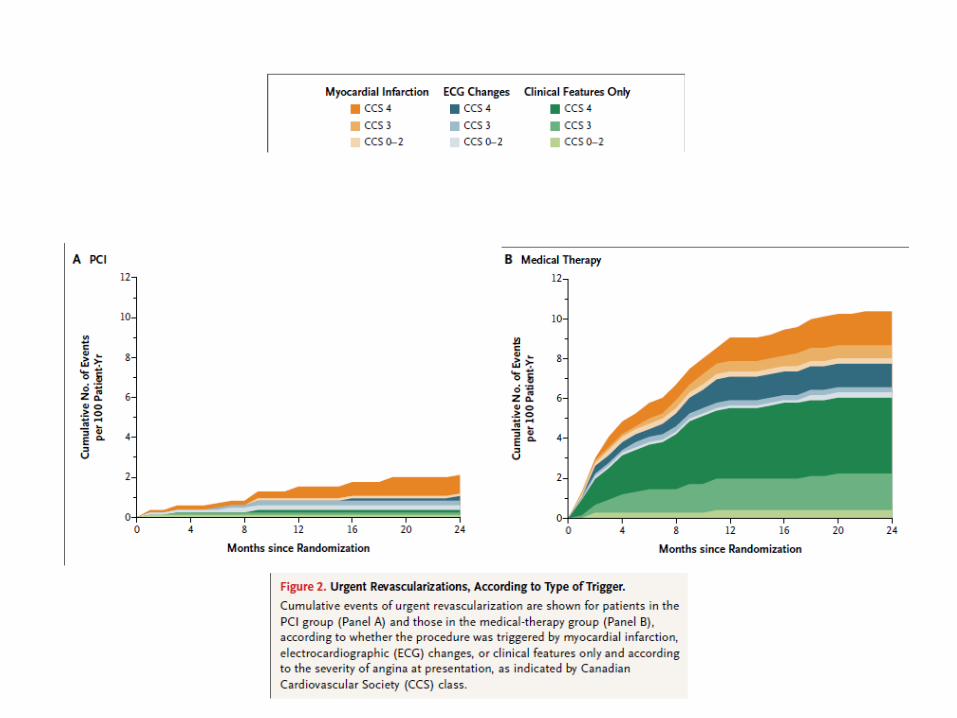
Discussão• Vários estudos sugerem que IAM peri-ACTP
não tem impacto no prognóstico a longo prazo.
• Angina severa estava presente em mais de 90% dos pacientes submetidos a revascularização urgente
• O uso de DES de 2ª geração favorece o prognóstico favorável em 2 anos do grupo ACTP e reflete a prática clínica diária
Conclusão
• Em pacientes com DAC estável, ACTP guiada por FFR melhora desfechos em 2 anos quando comparada com tratamento clínico isolado
• A melhora no prognóstico se deu principalmente às custas da redução da necessidade de revascularização urgente, mas também houve redução da incidência do desfecho combinado morte e infarto não-fatal.
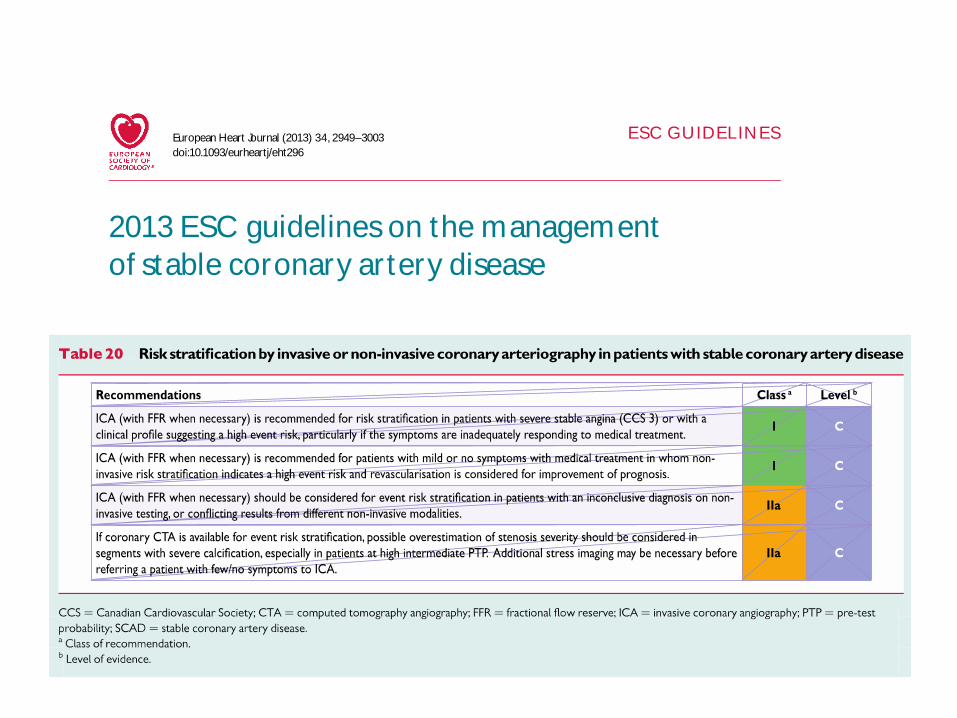
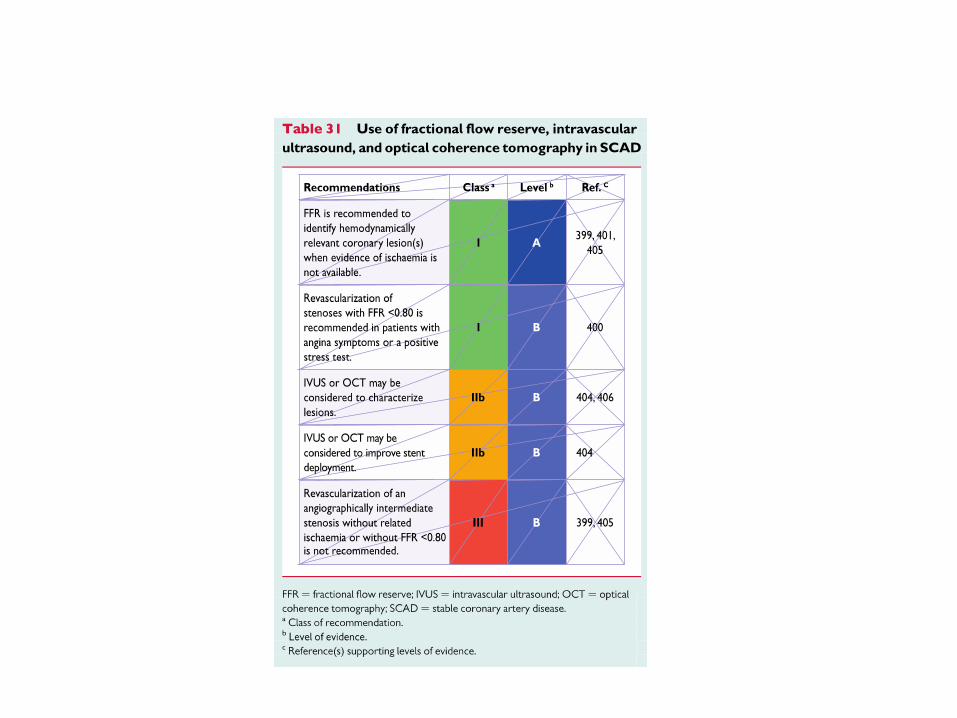
ESC GUIDELINES
2013 ESC guidelineson the managementof stable coronary artery diseaseThe Task Force on themanagement of stable coronary ar tery diseaseof the European Society of Cardiology
Task Force Members: GillesMontalescot * (Chairperson) (France), Udo Sechtem *
(Chairperson) (Germany), Stephan Achenbach (Germany), Felicita Andreot t i (Italy),Chr isArden (UK), Andrzej Budaj (Poland), Raffaele Bugiardini (Italy), Filippo Crea(Italy), ThomasCuisset (France), Car lo Di Mar io (UK), J. Rafael Ferreira (Por tugal ),Bernard J. Gersh (USA), Anselm K. Git t (Germany), Jean-Sebast ien Hulot (France),N ikolausMarx (Germany), Lionel H. Opie (South Afr ica), Mat thiasPfisterer(Switzer land), EvaPrescot t (Denmark), Frank Ruschitzka (Switzer land),Manel Sabat e(Spain), Roxy Senior (UK), David Paul Taggar t (UK), Ernst E. van der W all(Nether lands), Chr ist iaan J.M. Vr ints (Belgium).
ESC Commit tee for Pract ice Guidelines (CPG): Jose LuisZamorano (Chair person) (Spain), Stephan Achenbach(Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Nether lands), Hector Bueno (Spain), Veronica Dean(France), Chr ist i Deaton (UK), Cet in Erol (Turkey), Rober t Fagard (Belgium), Roberto Ferrar i (Italy), David Hasdai(Israel ), ArnoW .Hoes(Nether lands), PaulusKirchhof (Germany/UK), Juhani Knuut i (Finland), PhilippeKolh (Belgium),Patr izio Lancellot t i (Belgium), AlesLinhar t (Czech Republic), PetrosNihoyannopoulos(UK),Massimo F.Piepoli (Italy),Piot r Ponikowski (Poland), Per Anton Sirnes (Norway), Juan LuisTamargo (Spain), Michal Tendera (Poland),Adam Torbicki (Poland), W illiam W ijns (Belgium), Stephan W indecker (Switzer land).
Document Reviewers: Juhani Knuut i (CPG Review Coordinat or ) (Finland), Marco Valgimigli (Review Coordinator)(Italy), Hector Bueno (Spain), Marc J. Claeys (Belgium), Norber t Donner-Banzhoff (Germany), Cet in Erol (Turkey),Herber t Frank (Aust r ia), Chr ist ian Funck-Brentano (France), Oliver Gaemper li (Switzer land),Jose R. Gonzalez-Juanatey (Spain), Michalis Hamilos (Greece), David Hasdai (Israel ), Steen Husted (Denmark),Stefan K. James (Sweden), Kar i Kervinen (Finland), Philippe Kolh (Belgium), Steen Dalby Kr istensen (Denmark),Pat r izio Lancellot t i (Belgium), Aldo Piet ro Maggioni (Italy), Massimo F. Piepoli (Italy), Axel R. Pr ies (Germany),
* Correspondingauthors. The two chairmen contributed equally to thedocuments. Chairman, France: Professor GillesMontalescot, Institut deCardiologie,Pitie-Salpetriere UniversityHospital, Bureau 2-236, 47-83 Boulevard de l’Hopital, 75013Paris, France. Tel: + 33 142 163006, Fax: + 33 1 42 16 2931.Email: [email protected], Germany:Professor UdoSechtem,Abteilungfur Kardiologie,Robert BoschKrankenhaus,Auerbachstr.110,DE-70376Stuttgart,Germany.Tel: + 4971181013456,Fax:+ 4971181013795,Email:[email protected]
Entitieshavingparticipated in the development of thisdocument:
ESC Associations: Acute Cardiovascular Care Association (ACCA), European Association of Cardiovascular Imaging (EACVI), European Association for Cardiovascular Prevention &Rehabilitation (EACPR), European Association of PercutaneousCardiovascular Interventions (EAPCI), Heart Failure Association (HFA)
ESCWorkingGroups: Cardiovascular Pharmacology andDrugTherapy,Cardiovascular Surgery,Coronary Pathophysiology andMicrocirculation,Nuclear Cardiology andCardiacCT,Thrombosis, Cardiovascular Magnetic Resonance
ESC Councils: Cardiology Practice, Primary Cardiovascular Care
Thecontent of theseEuropean Society of Cardiology (ESC) Guidelines hasbeen published for personal and educational useonly.No commercial use isauthorized.No part of theESCGuidelinesmaybetranslatedor reproduced inany formwithout writtenpermissionfromtheESC.Permission canbeobtaineduponsubmissionofawrittenrequest toOxfordUniversityPress, the publisher of theEuropean Heart Journal and theparty authorized to handle such permissions on behalf of theESC.
Disclaimer .TheESCGuidelinesrepresent the viewsof theESC andwerearrived at after careful consideration of theavailable evidence at the time theywerewritten.Health profes-sionalsareencouraged to take them fully into account when exercising their clinical judgement. TheGuidelinesdo not, however, override the individual responsibility of health profes-sionalstomakeappropriatedecisionsinthecircumstancesof theindividual patients, inconsultationwiththat patient andwhereappropriateandnecessary thepatient’sguardianor carer. Itisalso the health professional’s responsibility to verify the rulesand regulationsapplicable to drugsand devicesat the time of prescription.
& TheEuropean Society of Cardiology 2013. All rights reserved. For permissionsplease email: [email protected]
European Heart Journal (2013) 34, 2949–3003doi:10.1093/eurheartj/eht296
by guest on June 30, 2014http://eurheartj.oxfordjournals.org/
Dow
nloaded from