Comparação das taxas de implantação entre a Injeção ... · publicada em 2010, comparando a...
56
AMANDA SETTI RAIZE Comparação das taxas de implantação entre a Injeção intracitoplasmática de espermatozoide morfologicamente selecionado (IMSI) e a injeção intracitoplasmática de espermatozoide (ICSI) em casais com falha prévia de ICSI ou fator masculino de infertilidade: uma meta-análise SÃO PAULO 2015 Dissertação apresentada ao Curso de Pós- Graduação da Faculdade de Ciências Médicas da Santa Casa de São Paulo para obtenção do título de Mestra em Ciências da Saúde.
Transcript of Comparação das taxas de implantação entre a Injeção ... · publicada em 2010, comparando a...

AMANDA SETTI RAIZE
Comparação das taxas de implantação entre a Injeção
intracitoplasmática de espermatozoide morfologicamente selecionado
(IMSI) e a injeção intracitoplasmática de espermatozoide (ICSI) em
casais com falha prévia de ICSI ou fator masculino de infertilidade:
uma meta-análise
SÃO PAULO
2015
Dissertação apresentada ao Curso de Pós-
Graduação da Faculdade de Ciências Médicas da
Santa Casa de São Paulo para obtenção do título de
Mestra em Ciências da Saúde.

�
�
AMANDA SETTI RAIZE
Comparação das taxas de implantação entre a Injeção
intracitoplasmática de espermatozoide morfologicamente selecionado
(IMSI) e a injeção intracitoplasmática de espermatozoide (ICSI) em
casais com falha prévia de ICSI ou fator masculino de infertilidade:
uma meta-análise
SÃO PAULO
2015
Dissertação apresentada ao Curso de Pós-
Graduação da Faculdade de Ciências Médicas da
Santa Casa de São Paulo para obtenção do título de
Mestra em Ciências da Saúde.
Orientador: Prof. Dr. Tsutomu Aoki
Co-orientador: Prof. Dr. Edson Borges Jr.
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
FICHA CATALOGRÁFICA
Preparada pela Biblioteca Central da Faculdade de Ciências Médicas da Santa Casa de São Paulo
Raize, Amanda Setti Comparação das taxas de implantação entre a injeção intracitoplasmática de espermatozoide morfologicamente selecionado (IMSI) e a injecção intracitoplasmática de espermatozoide (ICSI) em casais com falha prévia de ICSI ou fator masculino de infertilidade: uma meta-análise./ Amanda Setti Raize. São Paulo, 2015.
Dissertação de Mestrado. Faculdade de Ciências Médicas da Santa Casa de São Paulo – Curso de Pós-Graduação em Ciências da Saúde.
Área de Concentração: Ciências da Saúde Orientador: Tsutomu Aoki Co-Orientador: Edson Borges Junior
1. Infertilidade 2. Espermatozoides 3. Injeções de esperma intracitoplásmicas 4. Implantação do embrião 5. Gravidez 6. Perda do embrião
BC-FCMSCSP/46-15


�
�
DEDICATÓRIA
Dedico este trabalho ao meu pai, Carlos Augusto Setti, que me deu
a vida, educação, amizade, amor e suporte, incansavelmente. Eu devo
tudo a você.
�
�
AGRADECIMENTOS
A Deus – Laus Deo Semper
À minha mãe, Gloria Souza Setti (sempre presente), ao meu pai,
Carlos Augusto Setti e ao meu irmão, Rafael Souza Setti, por tudo que me
foi ensinado e proporcionado, pela confiança inabalável e pelo amor que
nunca faltou.
Ao meu marido, Luiz Raize Filho, por dividir comigo todas as
emoções da vida.
Às minhas melhores amigas, Adriana Farhat e Renata Lia Monteiro
Sierra pelos inúmeros momentos de descontração.
Ao meu orientador, Prof. Dr. Tsutomu Aoki, por todo o suporte no
mestrado e na elaboração deste trabalho.
Ao meu chefe e co-orientador, Prof. Dr. Edson Borges Jr., pelo
direcionamento e apoio constante na pesquisa científica, pela oportunidade
de realizar o mestrado e pelo suporte na elaboração deste trabalho.
Aos meus colegas de trabalho pelo companheirismo no dia-a-dia.
Especialmente à Daniela Paes de Almeida Braga Mattar por ter me
escolhido como parceira na pesquisa científica, por me ensinar grande
parte do que sei academicamente, pela amizade e parceria de sucesso que
conquistamos nesses seis anos.
À Faculdade de Ciências Médicas da Santa Casa de São Paulo e à
Pós Graduação da Faculdade de Ciências Médicas da Santa Casa de São
Paulo pela oportunidade e suporte durante o Mestrado.

�
�
À Coordenação de Aperfeiçoamento de Pessoal de Nível Superior
(CAPES) pela oportunidade e apoio financeiro durante o Mestrado.
�
�
LISTA DE ABREVIATURAS
ICSI – Injeção intracitoplasmática de espermatozoide
FIV – Fertilização in vitro
MSOME – Motile sperm organelle morphology examination
IMSI – Injeção intracitoplasmática de espermatozoide morfologicamente
selecionado
OR – Odds ratio
IC – Intervalo de confiança
�
�
LISTA DE FIGURAS
FIGURA 1: Espermatozoides visualizados sob magnificação de 400x. ............. 2�
FIGURA 2: Espermatozoides visualizados sob magnificação de 6.600x. .......... 4�
FIGURA 3: Espermatozoide contendo vacúolo nuclear visualizado sob
magnificação de 6.600x. .................................................................................... 5�

�
�
SUMÁRIO
1.� INTRODUÇÃO����������������������������������������������������������������������������������������������������
2.� OBJETIVOS��������������������������������������������������������������������������������������������������������
Objetivo geral�������������������������������������������������������������������������������������������������������������
Objetivos específicos������������������������������������������������������������������������������������������������
3.� MÉTODOS���������������������������������������������������������������������������������������������������������
3.1.� Pesquisa bibliográfica�������������������������������������������������������������������������������������������
3.2.� Seleção dos estudos e extração de dados��������������������������������������������������������
3.3.� Análise estatística��������������������������������������������������������������������������������������������������
4.� ARTIGOS PUBLICADOS���������������������������������������������������������������������������������
5.� CONSIDERAÇÕES FINAIS������������������������������������������������������������������������������
6.� CONCLUSÕES��������������������������������������������������������������������������������������������������
7.� REFERÊNCIAS BIBLOGRÁFICAS�����������������������������������������������������������������

�
�
1. INTRODUÇÃO
� �
��
�
�
Desde a sua introdução em 1992 (Palermo et al, 1992), a Injeção
Intracitoplasmática de Espermatozoide (ICSI), onde um espermatozoide móvel é
selecionado, imobilizado, aspirado com uma agulha de microinjeção e injetado no
citoplasma do oócito, tem sido amplamente utilizada para tratar a infertilidade e tem
sido o tratamento de escolha na presença de fator masculino de infertilidade.
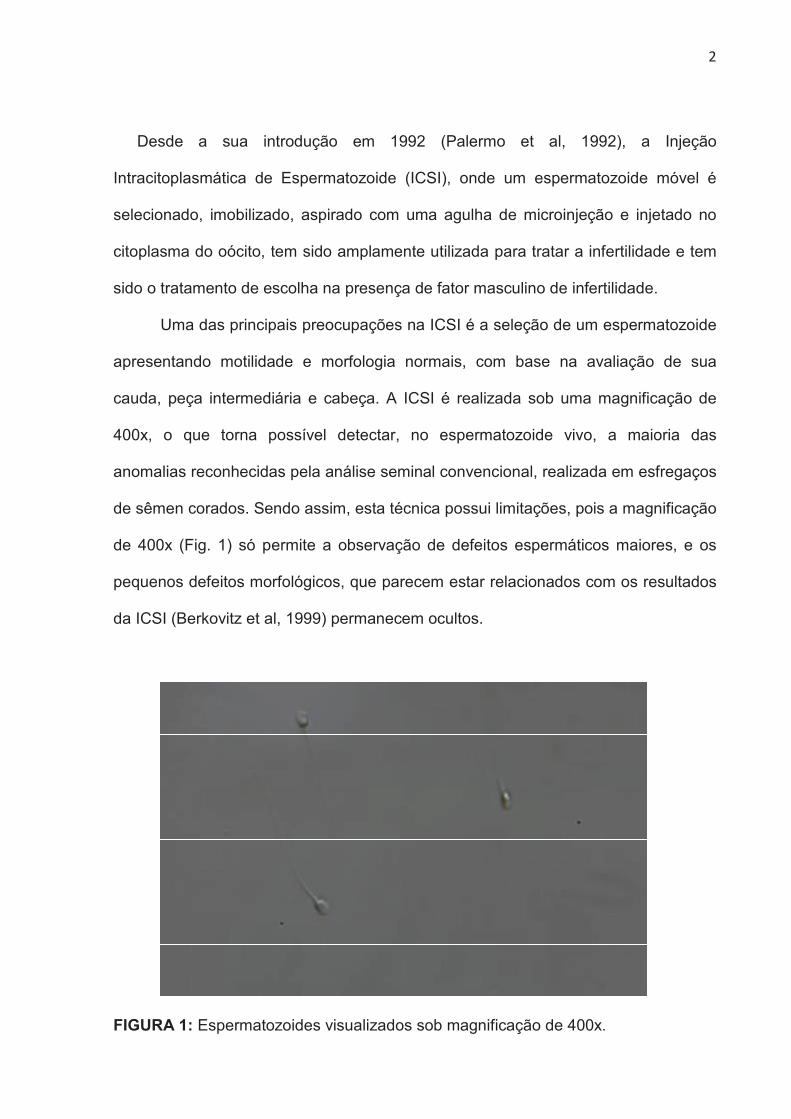
Uma das principais preocupações na ICSI é a seleção de um espermatozoide
apresentando motilidade e morfologia normais, com base na avaliação de sua
cauda, peça intermediária e cabeça. A ICSI é realizada sob uma magnificação de
400x, o que torna possível detectar, no espermatozoide vivo, a maioria das
anomalias reconhecidas pela análise seminal convencional, realizada em esfregaços
de sêmen corados. Sendo assim, esta técnica possui limitações, pois a magnificação
de 400x (Fig. 1) só permite a observação de defeitos espermáticos maiores, e os
pequenos defeitos morfológicos, que parecem estar relacionados com os resultados
da ICSI (Berkovitz et al, 1999) permanecem ocultos.
�
FIGURA 1: Espermatozoides visualizados sob magnificação de 400x.
��
�
Como conseqüência, os espermatozoides com aparência morfologicamente
normalsob este aumento podem, de fato, apresentar várias anormalidades
estruturais (Bartoov et al, 2002) que podem afetar negativamente o desenvolvimento
embrionário e o estabelecimento da implantação e gestação (Tesarik et al, 2002,
Tesarik, 2005). Este fato poderia explicar por que, apesar da vantagem de contornar
o fator masculino de infertilidade, os centros de reprodução assistida ainda
enfrentam o desafio de melhorar as taxa de gestação que permanecem em torno de
30-45%.
Inicialmente pensava-se que as taxas de sucesso da ICSI eram
independentes dos parâmetros seminais (Kupker et al, 1995, Mansour et al, 1995,
Nagy et al, 1995, Svalander et al, 1996, Lundin et al, 1997, Sukcharoen et al, 1998,
Zini et al, 2001). Muitos estudos tiveram como objetivo avaliar se há relação entre os
parâmetros seminais e os resultados da fertilização in vitro (FIV). A porcentagem de
espermatozoides morfologicamente normais foi reconhecida como o melhor preditor
de resultados para a inseminação intrauterina (Berkovitz et al, 1999) e FIV
convencional (Kruger et al, 1988, Liu and Baker, 1992, Mashiach et al, 1992). No
entanto, muitos estudos mostraram não haver relação entre a morfologia
espermática e os resultados da ICSI (Nagy et al, 1995, Svalander et al, 1996, Lundin
et al, 1997). Na tentativa de testar esta hipótese, um novo conceito deobservação de
espermatozoides em alta magnificação e em tempo real, conhecido como Avaliação
Morfológica das Organelas de Espermatozoides Móveis - do inglês Motile Sperm
Organelle Morphology Examination (MSOME), foi introduzido.
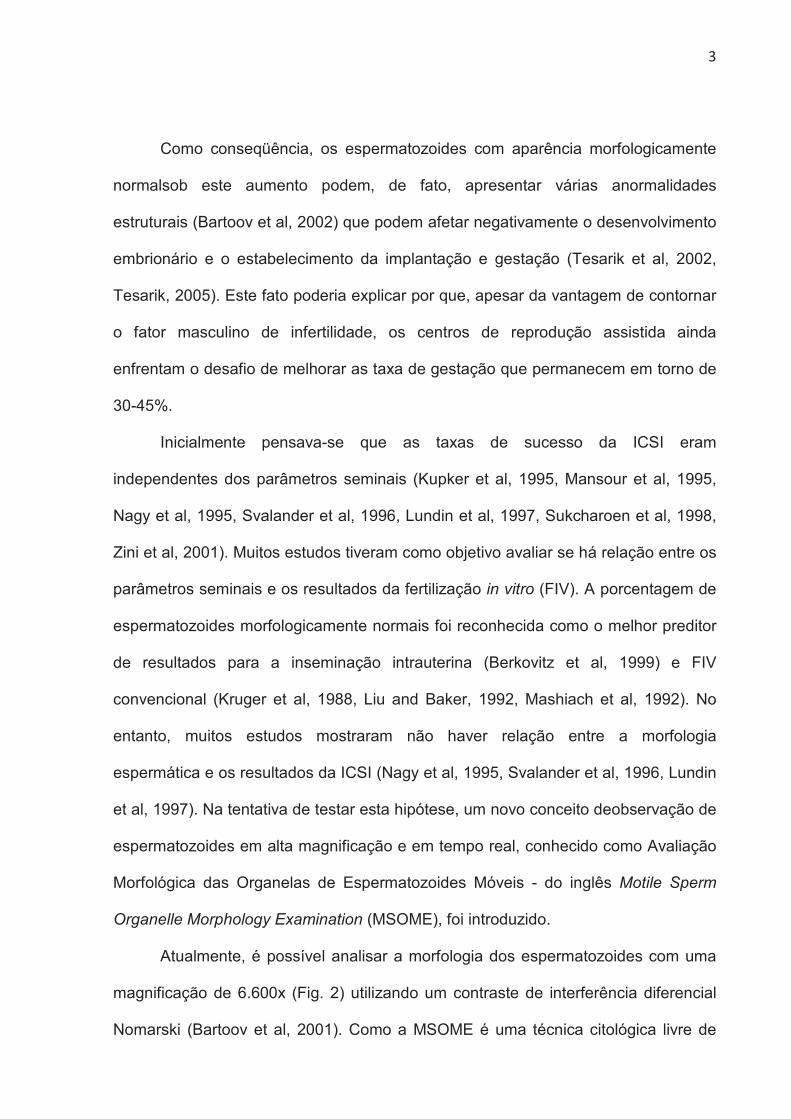
Atualmente, é possível analisar a morfologia dos espermatozoides com uma
magnificação de 6.600x (Fig. 2) utilizando um contraste de interferência diferencial
Nomarski (Bartoov et al, 2001). Como a MSOME é uma técnica citológica livre de
��
�
corantes, a sua incorporação, juntamente com um sistema de micromanipulação,
permitiu a introdução de um procedimento de ICSI modificado, conhecido como
Injeção Intracitoplasmática de Espermatozoides Morfologicamente Selecionados - do
inglês Intracytoplasmic Morphologically Selected Sperm Injection (IMSI). Como
conseqüência, a avaliação morfológica do espermatozoideem tempo real e em
magnificação variando de 6.600-13.000x (Garolla et al, 2008) permite a seleção dos
melhores espermatozoides móveis disponíveis antes da injeção.
�
FIGURA 2: Espermatozoides visualizados sob magnificação de 6.600x.
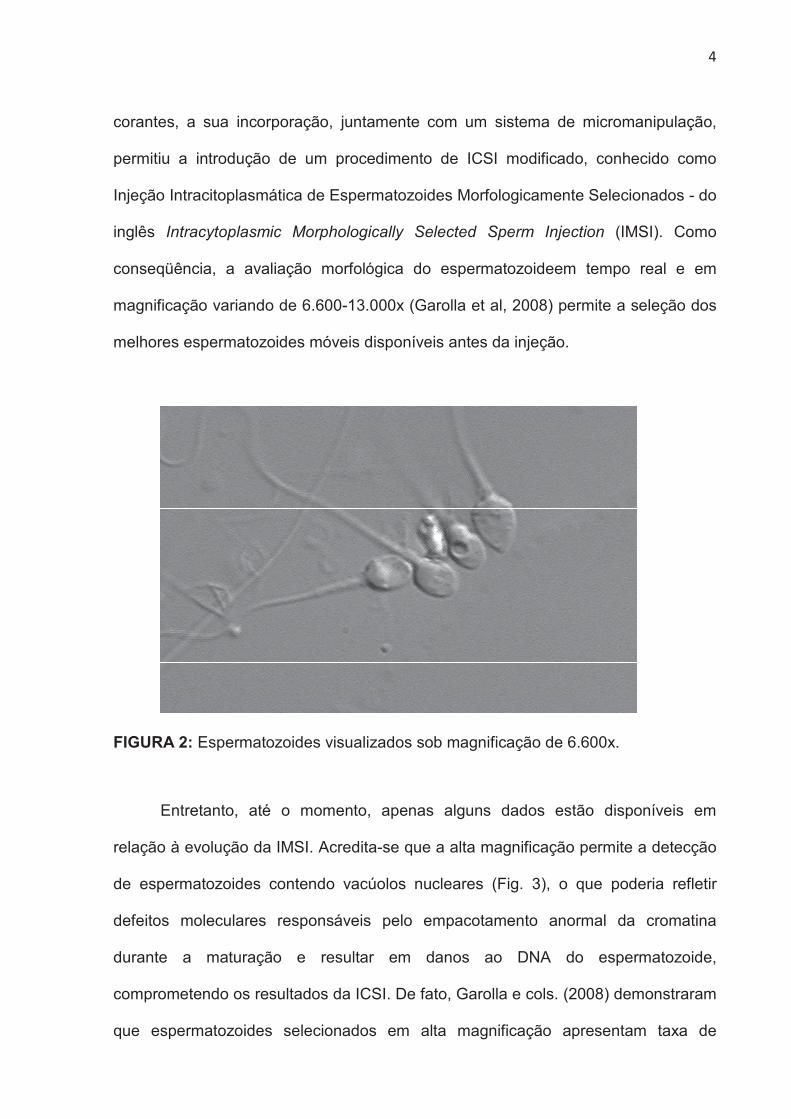
Entretanto, até o momento, apenas alguns dados estão disponíveis em
relação à evolução da IMSI. Acredita-se que a alta magnificação permite a detecção
de espermatozoides contendo vacúolos nucleares (Fig. 3), o que poderia refletir
defeitos moleculares responsáveis pelo empacotamento anormal da cromatina
durante a maturação e resultar em danos ao DNA do espermatozoide,
comprometendo os resultados da ICSI. De fato, Garolla e cols. (2008) demonstraram
que espermatozoides selecionados em alta magnificação apresentam taxa de

��
�
aneuploidia significativamente reduzida quando comparada à de espermatozoides
apresentando vacúolos. Ademais, o papel dos vacúolos nucleares de
espermatozoides foi abordado em outro estudo que demonstrou uma proporção
significativamente maior de fragmentação do DNA em espermatozoides
apresentando vacúolos do que em espermatozoides morfologicamente normais
(Franco et al, 2008). Ainda, outro estudo analisou o desenvolvimento embrionário
após a injeção de oócitos de mesma coorte com diferentes classes morfológicas de
espermatozoides avaliados sob alta magnificação (Vanderzwalmen and Fallet,
2008). Os autores relataram que a quantidade e o tamanho dos vacúolos nucleares
não comprometem a taxa de embriões de alta qualidade no dia-3, no entanto,
exercem um efeito negativo sobre o potencial de desenvolvimento do embrião até a
fase de blastocisto.
�
FIGURA 3: Espermatozoide contendo vacúolo nuclear visualizado sob magnificação
de 6.600x.
A aplicação da IMSI em pacientes previamente submetidos à FIV
convencional / ICSI vem demonstrando que uma investigação morfológica profunda
do espermatozoide favorece o sucesso do tratamento. Vários estudos mostraram
que a seleção de espermatozoides morfologicamente normais em alta magnificação
�
�
está positivamente associada com as taxas de implantação e gestação em casais
com falha de implantação prévia (Bartoov et al, 2003, Berkovitz et al, 2006,
Gonzalez-Ortega et al, 2010, Oliveira et al, 2011, El Khattabi et al, 2013, Klement et
al, 2013), fator masculino de infertilidade (Antinori et al, 2008, Balaban et al, 2011,
Knez et al, 2011, Oliveira et al, 2011, Setti et al, 2011, Wilding et al, 2011, Knez et al,
2012, De Vos et al, 2013, El Khattabi et al, 2013, Klement et al, 2013) e em
pacientes com um elevado grau de fragmentação do DNA dos espermatozoides.
(Hazout et al, 2006).
Sabe-se que o espermatozoide humano tem participação altamente dinâmica
e essencial na embriogênese que claramente vai além do processo de fertilização.
As primeiras divisões de embrião recém-formado dependem da maquinaria do
oócito, porém, a ativação do genoma embrionário ocorre na fase de 4-8 células.
Como resultado, os efeitos da injeção de espermatozoides com anormalidades
nucleares geralmente não são detectados antes do estágio de 8 células, quando
uma alta expressão de genes derivados do espermatozoide é iniciada. Os estudos
sugerem que este resultado reflete um efeito paterno tardio, que está relacionado ao
bloqueio do desenvolvimento embrionário observado durante ou após a implantação
de embriões com cariótipo normal (Tesarik et al, 2004, Borini et al, 2006).
Ainda, um recente estudo mostrou que a ICSI realizada com espermatozoides
livres de malformações nucleares está associada à incidência reduzida de
aneuploidia nos embriões resultantes (Figueira Rde et al, 2011). Portanto, um
espermatozoide morfologicamente anormal pode comprometer o embrião em
diferentes aspectos e momentos do seu desenvolvimento, afetar a implantação e
ocasionar a perda embrionária.
�
�
Apesar do crescente número de estudos demonstrando a eficácia da IMSI em
relação à utilização de espermatozoides morfologicamente normais, com melhor
empacotamento da cromatina e menor taxa de fragmentação do DNA, ainda se faz
necessária a identificação dos tipos de infertilidade que mais se beneficiam da
técnica.
A meta-análise fornece um consenso geral de estudos, resultando numa
estimativa mais precisa do que qualquer artigo individual. Uma meta-análise,
publicada em 2010, comparando a técnicas de ICSI e IMSI concluiu que a IMSI não
só melhora significativamente as taxas de embriões de boa qualidade, implantação e
gravidez, como também reduz significativamente as taxas de aborto, em
comparação com a ICSI (Souza Setti et al, 2010). No entanto, esta meta-análise
incluiu um único ensaio clínico randomizado e dois estudos não randomizados. Da
mesma forma, uma meta-análise mais recente mostrou que a IMSI melhora as taxas
de gestação clínica (Teixeira et al, 2013). Ambas as meta-análises não avaliaram os
diferentes fatores de infertilidade separadamente, portanto, seus resultados podem
não ser generalizados para todos os casais submetidos à FIV.

��
�
2. OBJETIVOS
�
��
�
Objetivo geral
Realizar uma meta-análise comparando os resultados clínicos da ICSI
e IMSI em casais com fator masculino de infertilidade e em casais com falha
prévia de ICSI.
Objetivos específicos
Comparar a influência da ICSI e IMSI nas seguintes variáveis clínicas:
(i) Taxa de implantação;
(ii) Taxa de gestação;
(iii) Taxa de aborto.

���
�
3. MÉTODOS
���
�
3.1. Pesquisa bibliográfica
�
A busca computadorizada foi realizada na base de dados COCHRANE,
MEDLINE, EMBASE, SCIELO (de janeiro de 2001 até Abril de 2013) para identificar
artigos relatando a comparação dos resultados de ICSI e IMSI. As palavras-chave
utilizadas foram: "intracytoplasmic morphologically selected sperm injection", "motile
sperm organelle morphology examination", "IMSI", "MSOME" e "high magnification
ICSI". A pesquisa não foi restrita a artigos escritos em Inglês. Não houve restrição
com relação ao desenho experimental dos estudos. As listas de referência dos
estudos elegíveis foram examinadas para identificação de possíveis artigos
adicionais.
3.2. Seleção dos estudos e extração de dados
�
Estudos não publicados, anais de congressos, teses de pós-graduação e
capítulos de livros não foram incluídos nesta meta-análise. Estudos que tratam de
azoospermia e fragmentação do DNA espermático e estudos em que pacientes
atuaram como seus próprios controles foram excluídos da análise. Os principais
desfechos foram as taxas de implantação, gestação e aborto. Os estudos foram
selecionados em um processo de duas fases. Na primeira fase, os títulos e resumos
das buscas eletrônicas foram analisados por dois revisores de forma independente.
Estudos não relevantes foram excluídos e os manuscritos de todas as citações que
possivelmente satisfizessem os critérios de seleção pré-definidos foram obtidos. Na
segunda fase, as decisões finais de inclusão ou exclusão foram feitas após a análise
dos manuscritos por ambos os revisores.
Os dados de todos os estudos elegíveis foram extraídos. Para cada estudo
foram registrados os seguintes dados: demográficos (autores, tipo de estudo, país
���
�
de origem, a idade média dos pacientes no momento da inscrição e período de
inscrição); procedimento (número de pacientes incluídos, critérios de inclusão e
exclusão para os pacientes das populações); e as taxas de implantação, gestação e
aborto dos tratamentos de ICSI e IMSI.
3.3. Análise estatística
�
Para cada estudo, os dados foram extraídos em tabelas 2x2. A medida de
heterogeneidade foi avaliada pelo teste I2. Para um resultado de I2 não significante o
modelo fixo foi utilizado. Para um resultado de I2 significante, um modelo aleatório foi
utilizado (DerSimonian e Laird). Os resultados foram analisados utilizando o modelo
estatístico de Mantel-Haenszel e estão expressos como odds ratio (OR), intervalos
de confiança de 95% (IC) e valor de p. A meta-análise foi realizada com o software
RevMan 5.2 (Colaboração Cochrane, Oxford, Reino Unido).
�

���
�
4. ARTIGOS PUBLICADOS
REVIEW
Twelve years of MSOME and IMSI: a review
Amanda Souza Setti a,b, Daniela Paes de Almeida Ferreira Braga a,b,Assumpto Iaconelli Jr a,b, Tsutomu Aoki c, Edson Borges Jr a,b,*
a Sapientiae Institute – Centro de Estudos e Pesquisa em Reproducao Humana Assistida, Rua Vieira Maciel, 62, Sao Paulo,SP 04503-040, Brazil; b Fertility – Centro de Fertilizacao Assistida, Av. Brigadeiro Luis Antonio, 4545, Sao Paulo,SP 01401-002, Brazil; c Faculdade de Ciencias Medicas da Santa Casa de Sao Paulo, Rua Dr. Cesario Motta Junior, 61,Sao Paulo, SP 01221-020, Brazil* Corresponding author. E-mail address: [email protected] (E Borges).
Amanda S. Setti obtained her BSc degree in 2005 at the University of Santo Amaro (UNISA) and specialized inhuman assisted reproduction in 2007 at the Sapientiae Institute. At present, she is a scientific researcher ofFertility – Centro de Fertilizacao Assistida and Instituto Sapientiae and a Master’s degree student at Faculdadede Ciencias Medicas da Santa Casa de Sao Paulo in Sao Paulo, Brazil.
Abstract A promising method for observing spermatozoa, motile sperm organelle morphology examination (MSOME) enables theevaluation of the nuclear morphology of motile spermatozoa in real time at high magnification and has allowed the introductionof a modified microinjection procedure, intracytoplasmic morphologically selected sperm injection (IMSI). Since its development,several studies have intensively investigated the efficacy of MSOME and IMSI. The objective of the present study is to review the
current literature on the MSOME and IMSI techniques. RBMOnline
ª 2013, Reproductive Healthcare Ltd. Published by Elsevier Ltd. All rights reserved.
KEYWORDS: ICSI, IMSI, MSOME, sperm morphology
Introduction
Since its introduction in 1992 (Palermo et al., 1992), intracy-toplasmic sperm injection (ICSI) has become the treatmentof choice in the presence of abnormal sperm parameters.In preparation for ICSI, the embryologist selects a spermato-zoon presenting both motility and normal morphology, basedon evaluation of its tail, neck and head. ICSI is usually per-formed under a magnification of ·400, which only enablesthe observation of major morphological defects. As a conse-quence, the selection of the ‘best-looking’ spermatozoon
may not represent the selection of a spermatozoon free ofmorphological abnormalities.
In the last decade, a new approach involving real-timehigh-magnification observation of unstained spermatozoa,motile sperm organelle morphology examination (MSOME),has been introduced (Bartoov et al., 2001). The incorpora-tion of this technique together with a micromanipulationsystem has allowed the introduction of a modified ICSI pro-cedure, intracytoplasmic morphologically selected sperminjection (IMSI). This system of real-time detailed morpho-logical sperm examination at high magnification, ranging
1472-6483/$ - see front matter ª 2013, Reproductive Healthcare Ltd. Published by Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.rbmo.2013.06.011
Reproductive BioMedicine Online (2013) 27, 338–352
www.sc iencedi rec t .comwww.rbmonl ine .com

from ·6600 to ·13,000 with Nomarski optics (Garolla et al.,2008), enables the selection of the best available motilespermatozoa before oocyte injection (Bartoov et al., 2001,2002, 2003; Berkovitz et al., 2006a,b).
Several publications have reported that IMSI is positivelyassociated with implantation and pregnancy rates (Bartoovet al., 2002, 2003; Berkovitz et al., 1999, 2005, 2006a,b;Hazout et al., 2006; Setti et al., 2011). However, the exactindications for IMSI are under debate. The objective of thisreview is to summarize the current literature on MSOME andIMSI.
MSOME
A physicist and optics theoretician, Georges Nomarski, iscredited with many inventions and patents, including amajor contribution to the renowned differential interfer-ence contrast microscopy technique in the mid-1950s. Alsoreferred to as Nomarski interference contrast, the methodallows transparent objects to be seen by using the differ-ence in the refraction of light when transmitted throughthe varying thicknesses of a specimen and provides a greaterdepth of focus allowing thicker specimens to be observedunder higher magnification (Ruzin, 1999).
Sperm morphological examination is performed under aninverted microscope equipped with high-power differentialinterference contrast. An aliquot of the prepared motilesperm fraction is transferred to a microdroplet of modifiedhuman tubal fluid medium containing polyvinyl pyrrolidonein a sterile glass-bottomed dish. The dish is placed on themicroscope stage above an Uplan Apo ·100 oil/·1.35 objec-tive lens that is previously covered by a droplet of immer-sion oil. The images are captured by a video camera,which has a 3-chip power charge-coupled device containingseveral effective picture elements (pixels) for high-qualityimage production, and a video monitor. The morphologicalassessment is conducted on the monitor screen which,under the above configuration, reaches a magnification thatis calculated based on four parameters: (i) objective magni-fication; (ii) magnification selector; (iii) video coupler mag-nification; and (iv) a calculated video magnification(Bartoov et al., 2001). In general, the total calculated mag-nification is ·6600 (objective magnification (·100) ·magnification selector (·1.5) · video coupler magnification(·0.99) · calculated video magnification (·355.6MM/8MM).
The MSOME assesses six sperm organelles: the acrosome,post-acrosomal lamina, neck, tail, mitochondria andnucleus. The acrosome and post-acrosomal lamina are con-sidered abnormal if absent, partial or vesiculated. Themitochondria should not be absent, partial or disorganized.The neck must not be abaxial nor should it contain disordersor cytoplasmic droplets, and the tail should not be coiled,broken, short or double (Bartoov et al., 2002, 2003). Amongthe six organelles, the sperm nucleus seems to be the mostimportant. According to the description given by Bartoovet al. (2002) the morphological normalcy of the spermnucleus is evaluated in terms of shape (smooth, symmetricand oval) and chromatin content (homogeneous chromatincontaining no more than one vacuole that occupies <4% ofthe nuclear area).
Sperm vacuoles: pathological or physiologicalevents?
Conventional light microscopic analysis of spermatozoa haslimitations in evaluating the fine structures, such as theacrosome and nucleus (Baccetti et al., 1996). The earlyultrastructural studies of human spermatozoa demonstratedthat the sperm nucleus often present at least one vacuole(Schultz-Larsen, 1958). The vacuole is a concavity extendingfrom the surface of the sperm head to the nucleus throughthe acrosome (Tanaka et al., 2012) that can be visualizedonly at a high magnification.
Recently, De Vos et al. (2013) aimed at documenting theprevalence of vacuoles in spermatozoa within a general ICSIpopulation. The study analysed 330 semen samples underhigh magnification and showed that approximately 18.1%of the spermatozoa were normally shaped and free of vacu-oles, 15.2% presented less than two small vacuoles, 12.3%displayed more than two small or at least one large vacuoleand 54.4% were grade IV, mainly because of being amor-phous in shape and/or presenting with large vacuoles. Theprevalence of vacuoles in normally shaped spermatozoawas as low as 27.5%. Nevertheless, it is important to empha-size that the magnification obtained in this study yielded amuch lower resolution than that obtained in other MSOMEstudies.
The origin of sperm vacuoles is disappointingly unknownand even after several investigations the question remains:are sperm vacuoles degenerative structures with no physio-logical importance or common physiologic features of thesperm head?
Some studies suggested that sperm vacuoles should beregarded as a normal feature of the sperm head (Chrzanow-ski, 1966; Fawcett, 1958; Pedersen, 1969; Tanaka et al.,2012), while others suggested that it is related to male sub-fertility (Mundy et al., 1994), lower mitochondrial mem-brane potential (Garolla et al., 2008), higher incidence ofchromosomal abnormalities (Garolla et al., 2008; Perdrixet al., 2011) and sperm chromatin packaging/DNA abnor-malities (Bartoov et al., 2001, 2002, 2003; Berkovitzet al., 2006a; Boitrelle et al., 2011; Cassuto et al., 2012;Franco et al., 2008, 2012; Oliveira et al., 2010a; Watanabeet al., 2011). It has also been suggested that sperm vacuolesreflect non-reacted acrosome (Kacem et al., 2011; Mont-jean et al., 2012) and therefore, the spermatozoa devoidfrom vacuoles selected through MSOME have undergoneacrosome reaction and are likely to induce oocyte activa-tion. Indeed, it has been demonstrated, in animal models,that the injection of spermatozoa with an intact acrosomeis potentially hazardous to embryo development (Morozumiand Yanagimachi, 2005).
Vacuoles and sperm maturation process
Recently, Tanaka et al. (2012) suggested that sperm vacu-oles are cavities in the nucleus that occur naturally duringthe process of sperm maturation, even in early stage sper-matids, and should not be considered as degenerative struc-tures. In addition, the authors pointed out that theincidence of vacuoles increased, but the size tended tobecome smaller, during the spermiogenesis and epididymaltransit. However, the authors highlighted that the size of
MSOME and IMSI: a review 339

the vacuoles is of importance and suggested that spermato-zoa with large vacuoles are not used for injection.
Vacuoles and acrosome reaction
A recent study investigated the nature of the nuclear vacu-oles (Kacem et al., 2011). As these vacuoles are localized atthe front of the sperm head the authors postulated thatthey might be of acrosomal origin. More than 3200 spermcells obtained from 30 semen samples from infertilepatients were evaluated regarding their acrosomalstatus using Pisum sativum agglutinin staining and MSOME.A significant difference in the proportion of sperm cellscontaining vacuoles was observed between spermatozoapresenting acrosomal material or intact acrosomesand acrosome-reacted spermatozoa (61.0% versus 29.0%).In addition, induction of the acrosomal reaction by iono-phore A23587 significantly increased the percentage of vac-uole-free spermatozoa from 41.2% to 63.8% and thepercentage of acrosome-reacted spermatozoa significantlyincreased from 17.4% to 36.1% (Kacem et al., 2011).
Montjean et al. (2012) evaluated 35 sperm samples thatwere incubated with the follicular fluid and with hyaluronicacid and analysed for sperm DNA condensation and morphol-ogy through MSOME, in order to determine if there was acorrelation between the presence of vacuoles and acrosomereaction. In accordance with the findings from Kacem et al.(2011), the results showed that the presence of sperm vac-uoles negatively influences sperm capacity to undergo acro-some reaction. The authors concluded that sperm vacuolesare a reflection of sperm physiology rather than an expres-sion of abnormalities in the nucleus.
Vacuoles and sperm DNA damage and chromosomal status
The human spermatozoon is crucial for contributing threecomponents: (i) the paternal genome; (ii) the signal to initi-ate oocyte activation; and (iii) the centriole; which partici-pates in the initial development of the zygote (Barrosoet al., 2009). In addition, the human spermatozoon playsan essential role in embryogenesis that goes beyond the fer-tilization process. The activation of the embryonic genomeat the stage of 4–8 cells depends on the expression of thepaternal genome (Braude et al., 1988). Studies suggest thatthe injection of DNA-damaged spermatozoa is related toblockage of embryonic development during/after theimplantation of embryos, which reflects a late paternaleffect (Borini et al., 2006; Tesarik et al., 2004).
Sperm DNA integrity and chromosomal constitution can-not be assessed in the sperm cell used for ICSI, thereforeseveral studies have investigated the relationship betweensperm morphology by MSOME and DNA fragmentation and/orsperm chromosomal status. The following studies evaluatingthe relationship between the presence of sperm vacuolesand chromatin and/or DNA and/or chromosomal abnormali-ties are summarized in Table 1.
Garolla et al. (2008) evaluated the correlation betweenDNA fragmentation and spermmorphology under high magni-fication (·13,000) in 10 patients with severe testicularimpairment. A total of 20 single immotile sperm cells perpatient were retrieved and classified on the basis of normalmorphology and absence (group A, 10 cells) or presence ofvacuoles (group B, 10 cells). The same cells were further
characterized as normal or pathological for DNA fragmenta-tion (terminal deoxyribonucleotidyl transferase-mediateddUTP nick-end labelling assay; TUNEL). The authors foundthat group A contained a lower percentage of DNA-frag-mented spermatozoa than group B. In addition, fluorescentin-situ hybridization (FISH) analysis showed that no chromo-somal alteration was present in normal sperm cells (group A).
Franco et al. (2008) evaluated the extent of DNA frag-mentation (TUNEL assay) and the presence of denatured sin-gle-stranded or normal double-stranded DNA (acridineorange fluorescence method) in spermatozoa with largenuclear vacuoles (LNV) selected by high magnification from30 patients. Spermatozoa with a normal nucleus (NN) andLNV were selected and placed on different slides. DNA frag-mentation in spermatozoa with LNV (29.1%) was signifi-cantly higher (P < 0.001) than in spermatozoa with NN(15.9%). Similarly, the percentage of denatured-strandedDNA in spermatozoa with LNV (67.9%) was significantlyhigher (P < 0.001) than in spermatozoa with NN (33.1%).
In a study by de Almeida Ferreira Braga et al. (2011),MSOME, sperm DNA fragmentation (TUNEL assay) and sperm(FISH) evaluations were performed in 200 sperm cells fromeach of 50 patients undergoing ICSI as a result of male infer-tility. The results showed that the presence of vacuoles andabnormal nuclear cell size observed via MSOME was posi-tively correlated with the incidence of sperm DNA fragmen-tation; however, the presence of sperm aneuploidy was notcorrelated with MSOME.
Wilding et al. (2011) assessed the correlation betweensperm morphology according to MSOME and DNA fragmenta-tion in 860 spermatozoa derived from eight separate analy-ses. The authors showed that only 331 of these spermatozoawere considered morphologically normal after MSOME. Ofthese, 4.2% were characterized as having fragmented DNAafter TUNEL assay. The study suggested a link betweenabnormal morphology after MSOME and the presence offragmented DNA, since only 14.4% of the spermatozoa pre-senting vacuoles after MSOME were found to contain frag-mented DNA, a significantly higher proportion ofspermatozoa than MSOME normal spermatozoa (P = 0.031).
Perdrix et al. (2011) assessed spermatozoa from neatsemen samples and spermatozoa presenting a vacuole occu-pying �13.0% total head area (spermatozoa with large vac-uole; SLV), isolated under high magnification (·6600) from20 patients with teratozoospermia. Both the neat samplesand SLV were evaluated for DNA fragmentation (TUNELassay), chromatin condensation (aniline blue staining) andsperm aneuploidy (FISH). The results showed that completeDNA fragmentation was significantly more frequent in nativespermatozoa than SLV, while chromatin condensation wassignificantly altered in SLV. In addition, aneuploidy and dip-loidy rates were significantly increased in SLV.
A recent study suggested that sperm head vacuoles arenot pathological or an indication of DNA damage and shouldbe considered as an ordinary characteristic in normal sper-matozoa (Watanabe et al., 2011). The study showed thatthe frequency of chromosomal alterations, which arederived from DNA fragmentation after fertilization, didnot differ significantly between motile normally shapedspermatozoa with a large vacuole and those without largevacuoles (9.1% versus 4.1%). In addition, the frequency ofchromosomal alterations was similar to that obtained for
340 AS Setti et al.
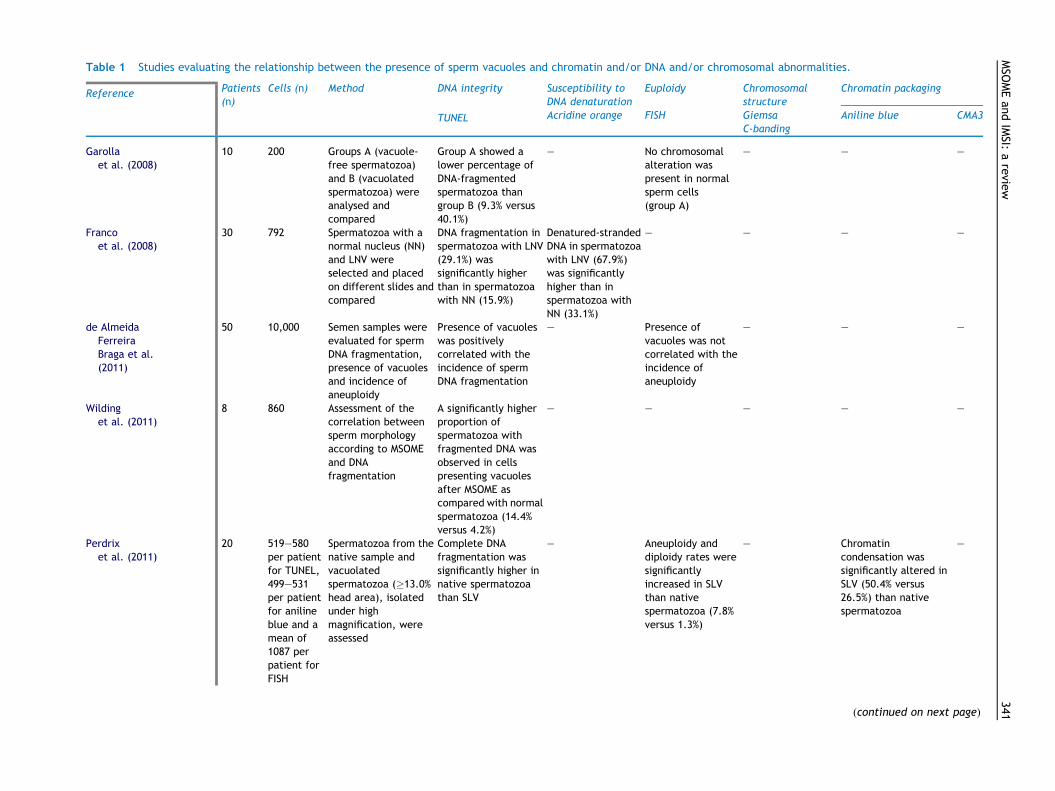
Table 1 Studies evaluating the relationship between the presence of sperm vacuoles and chromatin and/or DNA and/or chromosomal abnormalities.
Reference Patients(n)
Cells (n) Method DNA integrity Susceptibility toDNA denaturation
Euploidy Chromosomalstructure
Chromatin packaging
TUNEL Acridine orange FISH GiemsaC-banding
Aniline blue CMA3
Garollaet al. (2008)
10 200 Groups A (vacuole-free spermatozoa)and B (vacuolatedspermatozoa) wereanalysed andcompared
Group A showed alower percentage ofDNA-fragmentedspermatozoa thangroup B (9.3% versus40.1%)
– No chromosomalalteration waspresent in normalsperm cells(group A)
– – –
Francoet al. (2008)
30 792 Spermatozoa with anormal nucleus (NN)and LNV wereselected and placedon different slides andcompared
DNA fragmentation inspermatozoa with LNV(29.1%) wassignificantly higherthan in spermatozoawith NN (15.9%)
Denatured-strandedDNA in spermatozoawith LNV (67.9%)was significantlyhigher than inspermatozoa withNN (33.1%)
– – – –
de AlmeidaFerreiraBraga et al.(2011)
50 10,000 Semen samples wereevaluated for spermDNA fragmentation,presence of vacuolesand incidence ofaneuploidy
Presence of vacuoleswas positivelycorrelated with theincidence of spermDNA fragmentation
– Presence ofvacuoles was notcorrelated with theincidence ofaneuploidy
– – –
Wildinget al. (2011)
8 860 Assessment of thecorrelation betweensperm morphologyaccording to MSOMEand DNAfragmentation
A significantly higherproportion ofspermatozoa withfragmented DNA wasobserved in cellspresenting vacuolesafter MSOME ascompared with normalspermatozoa (14.4%versus 4.2%)
– – – – –
Perdrixet al. (2011)
20 519–580per patientfor TUNEL,499–531per patientfor anilineblue and amean of1087 perpatient forFISH
Spermatozoa from thenative sample andvacuolatedspermatozoa (�13.0%head area), isolatedunder highmagnification, wereassessed
Complete DNAfragmentation wassignificantly higher innative spermatozoathan SLV
– Aneuploidy anddiploidy rates weresignificantlyincreased in SLVthan nativespermatozoa (7.8%versus 1.3%)
– Chromatincondensation wassignificantly altered inSLV (50.4% versus26.5%) than nativespermatozoa
–
(continued on next page)
MSO
MEan
dIMSI:
arevie
w341
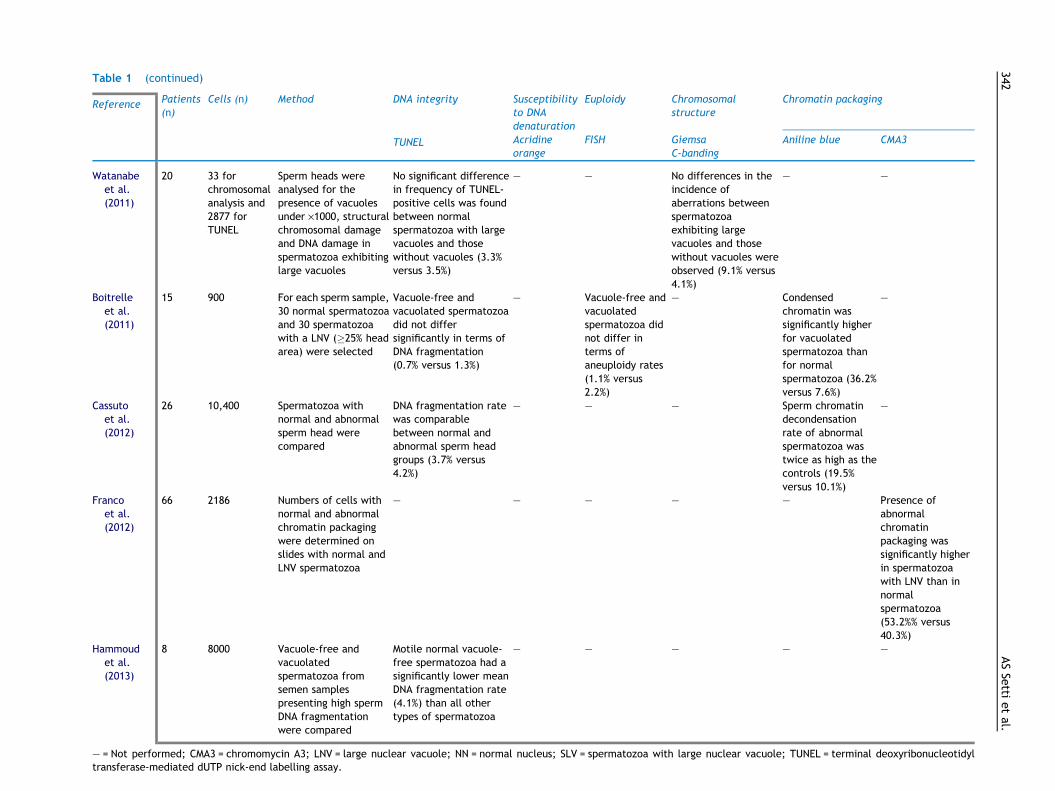
Table 1 (continued)
Reference Patients(n)
Cells (n) Method DNA integrity Susceptibilityto DNAdenaturation
Euploidy Chromosomalstructure
Chromatin packaging
TUNEL Acridineorange
FISH GiemsaC-banding
Aniline blue CMA3
Watanabeet al.(2011)
20 33 forchromosomalanalysis and2877 forTUNEL
Sperm heads wereanalysed for thepresence of vacuolesunder ·1000, structuralchromosomal damageand DNA damage inspermatozoa exhibitinglarge vacuoles
No significant differencein frequency of TUNEL-positive cells was foundbetween normalspermatozoa with largevacuoles and thosewithout vacuoles (3.3%versus 3.5%)
– – No differences in theincidence ofaberrations betweenspermatozoaexhibiting largevacuoles and thosewithout vacuoles wereobserved (9.1% versus4.1%)
– –
Boitrelleet al.(2011)
15 900 For each sperm sample,30 normal spermatozoaand 30 spermatozoawith a LNV (�25% headarea) were selected
Vacuole-free andvacuolated spermatozoadid not differsignificantly in terms ofDNA fragmentation(0.7% versus 1.3%)
– Vacuole-free andvacuolatedspermatozoa didnot differ interms ofaneuploidy rates(1.1% versus2.2%)
– Condensedchromatin wassignificantly higherfor vacuolatedspermatozoa thanfor normalspermatozoa (36.2%versus 7.6%)
–
Cassutoet al.(2012)
26 10,400 Spermatozoa withnormal and abnormalsperm head werecompared
DNA fragmentation ratewas comparablebetween normal andabnormal sperm headgroups (3.7% versus4.2%)
– – – Sperm chromatindecondensationrate of abnormalspermatozoa wastwice as high as thecontrols (19.5%versus 10.1%)
–
Francoet al.(2012)
66 2186 Numbers of cells withnormal and abnormalchromatin packagingwere determined onslides with normal andLNV spermatozoa
– – – – – Presence ofabnormalchromatinpackaging wassignificantly higherin spermatozoawith LNV than innormalspermatozoa(53.2%% versus40.3%)
Hammoudet al.(2013)
8 8000 Vacuole-free andvacuolatedspermatozoa fromsemen samplespresenting high spermDNA fragmentationwere compared
Motile normal vacuole-free spermatozoa had asignificantly lower meanDNA fragmentation rate(4.1%) than all othertypes of spermatozoa
– – – – –
– = Not performed; CMA3 = chromomycin A3; LNV = large nuclear vacuole; NN = normal nucleus; SLV = spermatozoa with large nuclear vacuole; TUNEL = terminal deoxyribonucleotidyltransferase-mediated dUTP nick-end labelling assay.
342ASSe
ttietal.

spermatozoa examined under ·400 magnification, suggest-ing that normal spermatozoa with DNA damage are not effi-ciently excluded by sperm selection under ·1000magnification (Watanabe et al., 2011). Nevertheless, it isnoteworthy that sperm morphology was examined under amagnification of ·1000 in this study, while in the majorityof studies a magnification of at least ·6000 was applied.
Boitrelle et al. (2011) used the MSOME (·10,000) toselect 450 normal spermatozoa and 450 spermatozoa witha large vacuole (�25% of the nuclear area) from semen sam-ples of 15 infertile patients and analysed chromatin conden-sation (aniline blue staining), DNA fragmentation (TUNEL)and chromosomal status (FISH X, Y, 18). The results showedthat the rate of non-condensed chromatin was significantlyhigher for vacuolated spermatozoa than for normal sperma-tozoa (36.2 ± 1.9% versus 7.6 ± 1.3%). The authors con-cluded that large vacuole appears to be a nuclear‘thumbprint’ linked to failure of chromatin condensation.
Cassuto et al. (2012) investigated whether chromatindamage (TUNEL and aniline blue assays) of 26 infertileman with oligoasthenoteratospermia and IVF failures waslinked with sperm-head abnormalities identified at highmagnification. The analysis of 10,400 spermatozoa showedthat the sperm chromatin-decondensation rate of abnormalspermatozoa (presenting abnormal head, presenting one orseveral vacuoles and an abnormal base) was twice as high asthe controls (19.5% versus 10.1%; P < 0.0001).
Franco et al. (2012) investigated the presence of abnor-mal sperm chromatin packaging in spermatozoa with LNV byanalysing the pattern of chromomycin A3 (CMA3) staining in66 men undergoing infertility diagnosis and treatment. Theauthors showed that the presence of CMA3-positive (abnor-mal) staining was significantly higher in spermatozoa withLNV than in CMA3-negative (normal) spermatozoa (53.2%versus 40.3%; P < 0.001, respectively).
Finally, Hammoud et al. (2013) analysed different typesof spermatozoa in eight patients with high degree of spermDNA fragmentation in terms of incidence of DNA fragmenta-tion. Vacuole-free spermatozoa showed a significantly lowerincidence of DNA fragmentation (4.1 ± 1.1%) than all othertypes of spermatozoa.
MSOME and conventional semen analysis
World Health Organization (WHO) reference values forhuman semen parameters are widely used to investigatemale reproductive potential. Evaluation of sperm morphol-ogy plays a crucial role in the diagnosis of male fertilitypotential and has demonstrated a predictive value forIVF–ICSI treatments (Kruger et al., 1986, 1987, 1988). How-ever, other authors found no relationship between spermmorphology and the success of ICSI (Host et al., 2001; Nagyet al., 1998; Oehninger et al., 1998).
MSOME provides an accurate description of spermatozoaabnormalities, particularly the presence of head vacuoles(Bartoov et al., 2002). However, no consensus has beenestablished concerning normal or abnormal MSOME criteria,despite being essential to transposing MSOME analysis intoroutine evaluation of male infertility (Perdrix et al., 2012).Some studies have analysed the relationship between spermnormalcy according to the WHO or Tygerberg criteria andMSOME.
Bartoov et al. (2002) investigated the relationshipbetween normal spermatozoa according to the WHO refer-ence values (WHO, 1999) and MSOME in 20 patients. Theauthors found no significant correlation between the per-centage of morphologically normal spermatozoa as definedby the WHO and the percentage of morphologically normalspermatozoa as defined by MSOME, since the incidence ofsperm normalcy by routine sperm analysis was significantlyhigher than that by MSOME (26.1 ± 7.2% and 2.9 ± 0.5%,respectively).
Oliveira et al. (2009) evaluated the correlation betweenMSOME classification and sperm morphology classificationaccording to the Tygerberg criteria (Kruger et al., 1986) in97 semen samples from an unselected group of couplesundergoing infertility investigation. The study showed astrong positive correlation between the percentage of nor-mal sperm forms according to the Tygerberg criteria andMSOME (r = 0.83; P < 0.001). However, MSOME was shownto be much more restrictive, presenting significantly lowernormality percentages for the semen samples in comparisonto those observed after analysis according to the Tygerbergcriteria (3 ± 3.2% versus 9.4 ± 4.8% respectively; P < 0.001).
In a previously mentioned study, Cassuto et al. (2012)observed significant correlations between the incidence ofscore-0 spermatozoa (presenting an abnormal head, oneor several vacuoles and an abnormal base) and sperm con-centration (r = �0.41), motility (r = �0.42) and morphology(r = �0.63).
Finally, Perdrix et al. (2012) analysed semen samplesfrom 440 males, aged between 24 and 66 years, consultingfor infertility investigation. One sample was obtained fromeach man and conventional semen analysis (WHO, 1999)andMSOME evaluation were performed simultaneously on thesame sample. A total of 109 men (24.8%) had normal semenparameters (normal group) and 331 men (75.2%) had at leastone abnormal semen parameter (abnormal group). MSOMEanalysis was performed on 10,975 spermatozoa. Sperm headvacuoles were significantly larger in abnormal semen sam-ples (P < 0.001). Relative vacuolar area (RVA), defined asvacuole area (lm2)/head area (lm2) ·100, was the most dis-criminative MSOME criterion between normal and abnormalsemen samples, and was negatively correlated with poorsperm morphology (r = 0.53; P < 0.001).
It is noteworthy that routine morphological examinationis applied to the entire semen sample, whereas the mostremarkable feature of MSOME is the focus on motile spermfractions, providing information about the sample fractionreferred for ICSI treatment. In addition, a recent study dem-onstrated that MSOME is a reliable technique for analysingsemen and supported the future use of MSOME as a routinemethod for semen analysis (Oliveira et al., 2010b).
MSOME and sperm preparation and manipulation
Given the importance of selecting a sperm preparationtechnique that minimizes possible paternal effects onembryo development by enhancing the sample with spermcells with few vacuoles, Monqaut et al. (2011) analysedsperm samples from 53 patients undergoing fertility treat-ment. Samples were analysed by high-magnification micros-copy before and after two preparation methods (swim-upand density gradient centrifugation) and classified according
MSOME and IMSI: a review 343

to the degree of vacuolization. Although both methodsshowed a positive effect on sperm quality, the swim-upmethod produced significantly higher increments of mor-phologically normal spermatozoa than gradient centrifuga-tion (59.3% versus 15.7%; P < 0.001).
It has previously been demonstrated that prolongedin-vitro incubation at 37�C may reduce sperm viability (Cal-amera et al., 2001). Since the morphological evaluation ofspermatozoa under high magnification is a time-consumingprocedure (Berkovitz et al., 2005) that should be conductedat 37�C, the inventors of MSOME investigated the impact ofincubation at 37�C on the morphological normalcy of thesperm nucleus (Peer et al., 2007).The study showed thatafter 2 h of incubation at 37�C, there was a significantincrease in the frequency of vacuolated nuclei (80.8 ± 7.2%versus 75.0 ± 7.6%; P < 0.01). No significant morphologicalchanges in sperm nuclei were observed upon prolongedincubation at 21�C. Finally, after 2 h of incubation, the inci-dence of spermatozoa with vacuolated nuclei was signifi-cantly higher at 37�C compared with 21�C (56.5 ± 10.8%versus 45.5 ± 10.0%; P < 0.01).
MSOME and male age
A recent study investigated the influence of paternal age onsperm quality by MSOME. Two hundred sperm cells from 975patients were analysed at ·8400 magnification (Silva et al.,2012) and the percentage of normal and LNV spermatozoawas determined. The subjects were divided into threegroups according to paternal age. The study demonstrateda significantly lower percentage of normal spermatozoa inthe older group (�41 years) compared with the youngergroups (�35 years and 36–40 years). In addition, the pro-portion of LNV spermatozoa was significantly higher in theolder group, while regression analysis demonstrated that a1-year increment in paternal age increased the incidenceof spermatozoa with LNV by 10%. This correlation was cor-roborated by findings obtained by de Almeida Ferreira Bragaet al. (2011).
MSOME and cryopreservation
It has previously been demonstrated that human spermcryopreservation is associated with alterations in spermmotility, viability and morphology (O’Connell et al., 2002).Boitrelle et al. (2012) investigated the potential value ofIMSI for frozen–thawed spermatozoa, and the current studygroup used MSOME, chromatin condensation assessment(aniline blue staining) and viability assessment (eosin per-meability) before and after freezing–thawing to assess therelationship between cryopreservation and potentialnuclear alterations in spermatozoa. The results showed thatcryopreservation decreases the percentage of morphologi-cally normal spermatozoa and viability rate and increasesthe proportion of spermatozoa with non-condensedchromatin.
Conclusions
The reason for the occurrence of vacuoles in the sperm headis yet to be elucidated and requires further studies. Several
studies have investigated the origin of this feature and theresults are controversial. Nonetheless, only two studiesshowed that there is no relationship between sperm nuclearvacuoles and sperm function; however, it is important toemphasize that one of these studies was an unpoweredinvestigation (Tanaka et al., 2012) and the other evaluatedsperm cells at ·1000 (Watanabe et al., 2011). The remainingstudies agreed that sperm nuclear vacuoles are eitherrelated to acrosome reaction, chromosomal status, chroma-tin condensation or DNA fragmentation.
Both studies that investigated the relation betweensperm vacuoles and acrosome reaction agreed that thereis a negative relation between the presence of vacuolesand the sperm capacity to undergo acrosome reaction.Therefore, the MSOME selection could be a tool for the elim-ination of the acrosome reaction-resistant spermatozoa.Regarding sperm DNA fragmentation, from nine studies,six reported that vacuole-free spermatozoa yields lowerrates of DNA fragmentation as compared with vacuolatedspermatozoa. It is important to emphasize that the TUNELassay was the method of choice in all these studies, whichcould have reduced the occurrence of bias. As for chromatinstatus, a negative correlation between the incidence of vac-uoles and chromatin condensation was observed in all theconducted studies (one study used CMA3 and three used ani-line blue staining). Finally, it seems that sperm aneuploidyis not related to the presence of vacuoles, nevertheless,one study observed increased rates of aneuploidy and dip-loidy in SLV.
According to De Vos et al. (2013), the prevalence of vac-uoles in normally shaped spermatozoa seems to be low. Inaddition, the use of ‘second-best’ spermatozoa appears tohave no implications on fertilization and embryo develop-ment. Nevertheless, it has been reported that up to 65%spermatozoa deemed suitable for ICSI by conventionalmethods were subsequently deselected after high-magnifi-cation analysis (Wilding et al., 2011)
Although the process of finding spermatozoa withoutvacuoles is difficult and time consuming and requires highlyskilled laboratory personnel, so far, the majority of thestudies suggest that there is a link between the presenceof vacuoles and sperm function, either with the acrosomereaction, chromatin condensation or DNA integrity. Moreimportantly, the SLV seems to be the most compromisedspermatozoa and should not be used for injection.
IMSI
MSOME followed by ICSI is a novel technique that involvesprolonged sperm manipulation (Berkovitz et al., 2005) andspecial instrumentation with considerable costs. In addi-tion, the technique requires a high level of technical exper-tise and inter-observer reproducibility (Said and Land,2011). A meta-analysis comparing ICSI versus IMSI outcomesconcluded that IMSI not only significantly improves the per-centage of top-quality embryos, implantation and preg-nancy rates, but also significantly reduces miscarriagerates as compared with ICSI (Souza Setti et al., 2010). Thesefindings can be explained by the fact that during ICSI mor-phological assessment of the sperm nucleus takes place at·400. Wilding et al. (2011) performed a mock ICSI trial to
344 AS Setti et al.
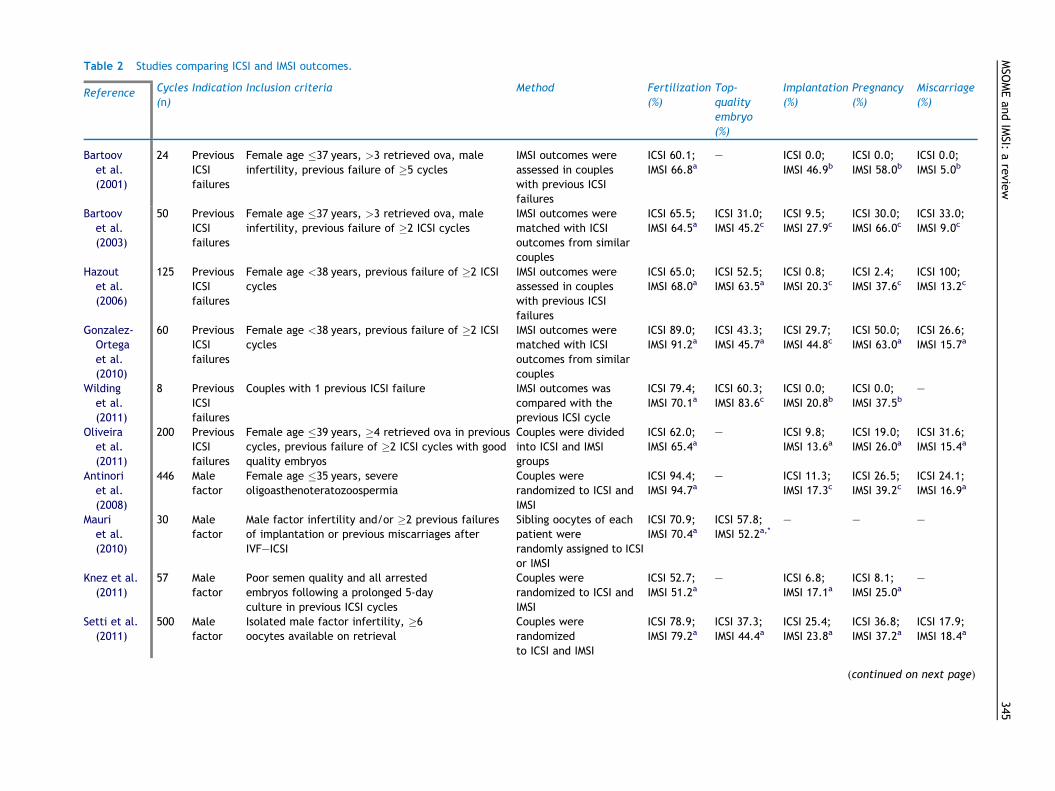
Table 2 Studies comparing ICSI and IMSI outcomes.
Reference Cycles(n)
Indication Inclusion criteria Method Fertilization(%)
Top-qualityembryo(%)
Implantation(%)
Pregnancy(%)
Miscarriage(%)
Bartoovet al.(2001)
24 PreviousICSIfailures
Female age �37 years, >3 retrieved ova, maleinfertility, previous failure of �5 cycles
IMSI outcomes wereassessed in coupleswith previous ICSIfailures
ICSI 60.1;IMSI 66.8a
– ICSI 0.0;IMSI 46.9b
ICSI 0.0;IMSI 58.0b
ICSI 0.0;IMSI 5.0b
Bartoovet al.(2003)
50 PreviousICSIfailures
Female age �37 years, >3 retrieved ova, maleinfertility, previous failure of �2 ICSI cycles
IMSI outcomes werematched with ICSIoutcomes from similarcouples
ICSI 65.5;IMSI 64.5a
ICSI 31.0;IMSI 45.2c
ICSI 9.5;IMSI 27.9c
ICSI 30.0;IMSI 66.0c
ICSI 33.0;IMSI 9.0c
Hazoutet al.(2006)
125 PreviousICSIfailures
Female age <38 years, previous failure of �2 ICSIcycles
IMSI outcomes wereassessed in coupleswith previous ICSIfailures
ICSI 65.0;IMSI 68.0a
ICSI 52.5;IMSI 63.5a
ICSI 0.8;IMSI 20.3c
ICSI 2.4;IMSI 37.6c
ICSI 100;IMSI 13.2c
Gonzalez-Ortegaet al.(2010)
60 PreviousICSIfailures
Female age <38 years, previous failure of �2 ICSIcycles
IMSI outcomes werematched with ICSIoutcomes from similarcouples
ICSI 89.0;IMSI 91.2a
ICSI 43.3;IMSI 45.7a
ICSI 29.7;IMSI 44.8c
ICSI 50.0;IMSI 63.0a
ICSI 26.6;IMSI 15.7a
Wildinget al.(2011)
8 PreviousICSIfailures
Couples with 1 previous ICSI failure IMSI outcomes wascompared with theprevious ICSI cycle
ICSI 79.4;IMSI 70.1a
ICSI 60.3;IMSI 83.6c
ICSI 0.0;IMSI 20.8b
ICSI 0.0;IMSI 37.5b
–
Oliveiraet al.(2011)
200 PreviousICSIfailures
Female age �39 years, �4 retrieved ova in previouscycles, previous failure of �2 ICSI cycles with goodquality embryos
Couples were dividedinto ICSI and IMSIgroups
ICSI 62.0;IMSI 65.4a
– ICSI 9.8;IMSI 13.6a
ICSI 19.0;IMSI 26.0a
ICSI 31.6;IMSI 15.4a
Antinoriet al.(2008)
446 Malefactor
Female age �35 years, severeoligoasthenoteratozoospermia
Couples wererandomized to ICSI andIMSI
ICSI 94.4;IMSI 94.7a
– ICSI 11.3;IMSI 17.3c
ICSI 26.5;IMSI 39.2c
ICSI 24.1;IMSI 16.9a
Mauriet al.(2010)
30 Malefactor
Male factor infertility and/or �2 previous failuresof implantation or previous miscarriages afterIVF–ICSI
Sibling oocytes of eachpatient wererandomly assigned to ICSIor IMSI
ICSI 70.9;IMSI 70.4a
ICSI 57.8;IMSI 52.2a,*
– – –
Knez et al.(2011)
57 Malefactor
Poor semen quality and all arrestedembryos following a prolonged 5-dayculture in previous ICSI cycles
Couples wererandomized to ICSI andIMSI
ICSI 52.7;IMSI 51.2a
– ICSI 6.8;IMSI 17.1a
ICSI 8.1;IMSI 25.0a
–
Setti et al.(2011)
500 Malefactor
Isolated male factor infertility, �6oocytes available on retrieval
Couples wererandomizedto ICSI and IMSI
ICSI 78.9;IMSI 79.2a
ICSI 37.3;IMSI 44.4a
ICSI 25.4;IMSI 23.8a
ICSI 36.8;IMSI 37.2a
ICSI 17.9;IMSI 18.4a
(continued on next page)
MSO
MEan
dIMSI:
arevie
w345
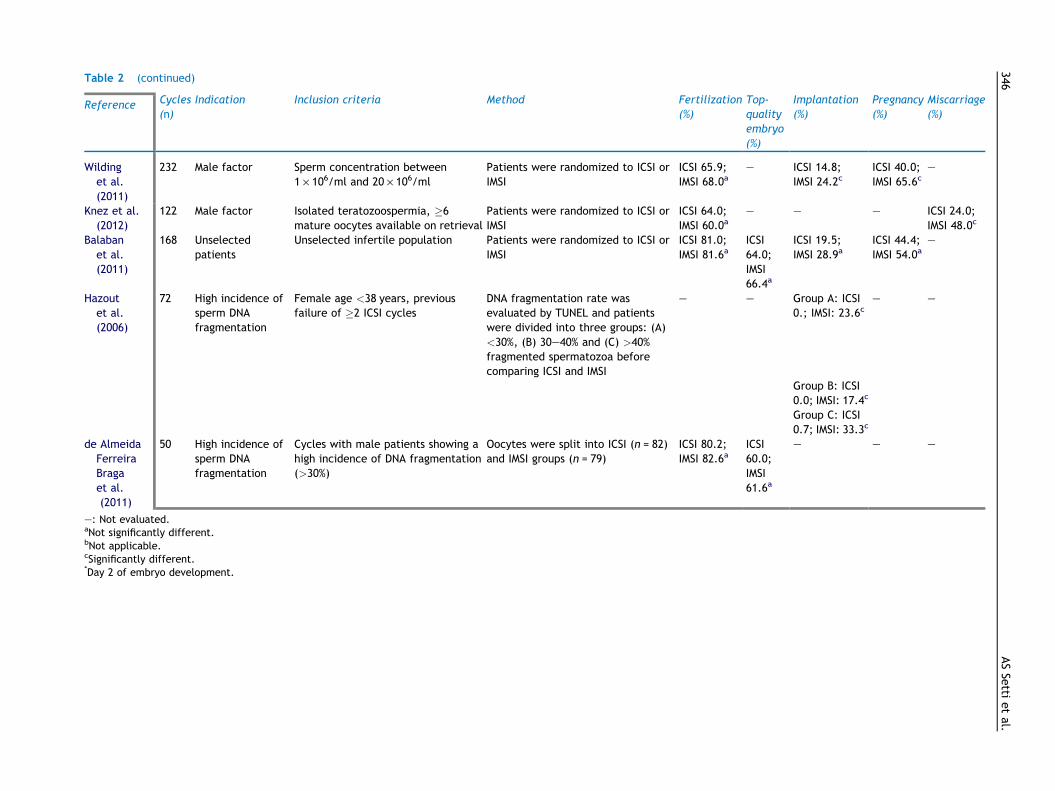
Table 2 (continued)
Reference Cycles(n)
Indication Inclusion criteria Method Fertilization(%)
Top-qualityembryo(%)
Implantation(%)
Pregnancy(%)
Miscarriage(%)
Wildinget al.(2011)
232 Male factor Sperm concentration between1 · 106/ml and 20 · 106/ml
Patients were randomized to ICSI orIMSI
ICSI 65.9;IMSI 68.0a
– ICSI 14.8;IMSI 24.2c
ICSI 40.0;IMSI 65.6c
–
Knez et al.(2012)
122 Male factor Isolated teratozoospermia, �6mature oocytes available on retrieval
Patients were randomized to ICSI orIMSI
ICSI 64.0;IMSI 60.0a
– – – ICSI 24.0;IMSI 48.0c
Balabanet al.(2011)
168 Unselectedpatients
Unselected infertile population Patients were randomized to ICSI orIMSI
ICSI 81.0;IMSI 81.6a
ICSI64.0;IMSI66.4a
ICSI 19.5;IMSI 28.9a
ICSI 44.4;IMSI 54.0a
–
Hazoutet al.(2006)
72 High incidence ofsperm DNAfragmentation
Female age <38 years, previousfailure of �2 ICSI cycles
DNA fragmentation rate wasevaluated by TUNEL and patientswere divided into three groups: (A)<30%, (B) 30–40% and (C) >40%fragmented spermatozoa beforecomparing ICSI and IMSI
– – Group A: ICSI0.; IMSI: 23.6c
– –
Group B: ICSI0.0; IMSI: 17.4c
Group C: ICSI0.7; IMSI: 33.3c
de AlmeidaFerreiraBragaet al.(2011)
50 High incidence ofsperm DNAfragmentation
Cycles with male patients showing ahigh incidence of DNA fragmentation(>30%)
Oocytes were split into ICSI (n = 82)and IMSI groups (n = 79)
ICSI 80.2;IMSI 82.6a
ICSI60.0;IMSI61.6a
– – –
–: Not evaluated.aNot significantly different.bNot applicable.cSignificantly different.*Day 2 of embryo development.
346ASSe
ttietal.

determine the proportion of spermatozoa, otherwiseselected for ICSI, that had morphological abnormalities.The results showed that 64.8% of the analysed spermatozoawere deselected after digital analysis. Reasons for rejectionof spermatozoa included poor morphology, the presence ofmultiple vacuoles, the presence of vacuoles that occupied>4% of the nuclear area and poor morphology of the mid-piece. The study suggested that selection of spermatozoaunder high magnification reveals morphological featuresnot visible using the conventional ICSI procedure and des-elects spermatozoa otherwise selected for ICSI.
Cassuto et al. (2009) retrospectively evaluated 27 cou-ples with male factor infertility referred for ICSI treatmentin order to establish a classification score for the spermato-zoon with the highest predictive fertilizing potential in realtime under a magnification of ·6100. The authors suggestedthe following formula for a morphologically ‘normal top‘spermatozoon: (normal head score = 2) + (lack of vacuolescore = 3) + (normal base score = 1). In women aged�30 years, the authors recommended using spermatozoawith a score of 4–6 for injection. In younger patients, scor-ing is not as critical, at least with regards to fertilization.
Several studies have investigated the benefits of IMSI bycomparing the results obtained using this technique withthose obtained via ICSI. The results are controversial andare described below according to the type of infertility(Table 2).
IMSI indications
IMSI in cases of previous IVF–ICSI failure
In a preliminary study, Bartoov et al. (2001) assessed 24couples in which the woman was <37 years old, with previ-ous failure of at least five consecutive cycles of IVF and ICSI,who had undergone a single cycle of IMSI, with at least threeoocytes retrieved, as a result of male infertility. The studyshowed that after IMSI, the pregnancy rate was 58%, theimplantation rate was 47% and the miscarriage rate was 5%.
In a continuation of the aforementioned study, Bartoovet al. (2003) investigated whether microinjection of motilespermatozoa with morphologically normal nuclei improvedthe pregnancy rate in 50 couples with repeated ICSI failures.After a single IMSI procedure, the couples were matchedwith couples who had undergone a routine ICSI procedureand experienced the same number of previous ICSI failures.The study revealed that fertilization and the proportion oftop-quality embryos were similar, but that the pregnancyrate in the IMSI group was significantly higher than that inthe ICSI group (66.0% versus 30.0%; P < 0.01) and the mis-carriage rate was significantly lower in the IMSI group (33.0%versus 9.0%; P < 0.01).
Hazout et al. (2006) evaluated the efficacy of IMSI in 125couples with at least two repeated ICSI failures in which thewoman was <38 years old. The results showed that fertiliza-tion, cleavage and top-quality embryo rates were similar inthe two previous ICSI attempts and sequential IMSI attempt.However, improved clinical outcomes such as pregnancy(37.6% versus 2.4%), implantation (20.3% versus 0.8%), deliv-ery (33.6% versus 0.0%) and birth rates (17.6% versus 0.0%)were observed in IMSI attempts compared with ICSI(P < 0.001), respectively.
Gonzalez-Ortega et al. (2010) compared the results of 30IMSI cycles performed in couples with at least two previousICSI failures and female age <38 years, and 30 ICSI cyclesperformed in couples with similar characteristics. The datashowed a significant difference in implantation rate infavour of IMSI (44.8% versus 29.7%). Although not signifi-cantly different, the pregnancy rate tended to be higherin IMSI cycles (63% versus 50%), demonstrating a trend infavour of IMSI.
Wilding et al. (2011) compared embryo quality obtainedafter IMSI in eight couples with their previous ICSI cycle. Theresults showed a significant difference in embryo qualitybetween the ICSI and IMSI cycles (60.3% versus 83.6%,respectively). In the same study the authors performed aprospective randomized trial involving couples undergoingICSI (n = 110) and IMSI (n = 122). The authors noted a signif-icantly higher percentage of high-quality embryos trans-ferred (66.0% versus 98.6%) and higher rates ofimplantation (14.8% versus 24.2%) and pregnancy (40.0%versus 65.6%) after IMSI.
Oliveira et al. (2011) compared the outcomes of ICSI andIMSI in 200 couples with at least two repeated ICSI failures.The study revealed trends toward lower rates of miscarriage(15.4% versus 31.6%), higher rates of ongoing pregnancy(22.0% versus 13.0%) and live birth (21.0% versus 12.0%) inthe IMSI group compared with the ICSI group. The study alsoanalysed subpopulations with or without male factors, andsimilar results to those obtained with the whole populationwere observed.
IMSI in cases of male factor infertility
Antinori et al. (2008) assessed the advantages of IMSI overconventional ICSI in the treatment of 446 couples withsevere oligoasthenoteratozoospermia and female age under35 years in a prospective randomized trial. The coupleswere randomized into ICSI (n = 219) and IMSI (n = 227)groups. The results showed that IMSI resulted in a higherpregnancy rate (39.2% versus 26.5%; P = 0.004) comparedwith ICSI. In addition, the study demonstrated that patientswith two or more previous ICSI failures benefited the mostfrom IMSI in terms of pregnancy rate (29.8% versus 12.9%;P = 0.017).
Mauri et al. (2010) evaluated whether IMSI could influ-ence early paternal effects by observing embryo quality atday 2 in 30 couples with male factor infertility and/or atleast two previous failures of implantation and/or previousmiscarriages after IVF–ICSI. The results obtained using sib-ling oocytes showed that ICSI and IMSI provided a similarproportion of top-quality embryos.
Knez et al. (2011) compared the results obtained withICSI (37 couples) and IMSI (20 couples) in couples with poorsemen quality and all embryos arrested after culture to theblastocyst stage in their previous ICSI attempts in a prospec-tive randomized study. The outcomes of current cycles werecompared with the outcomes of the previous ICSI cycles.The IMSI group showed a higher number of blastocysts (0.80versus 0.65) and lower number of cycles without embryotransfer (0% versus 27.0%, P = 0.048) compared with the ICSIgroup. A trend toward higher implantation (17.1% versus6.8%) and pregnancy rates (25.0% versus 8.1%) was observedin the IMSI group.
MSOME and IMSI: a review 347

Setti et al. (2011), in a prospective randomized study,compared ICSI and IMSI outcomes in 500 couples with malefactor infertility and at least six retrieved oocytes. Theresults showed that the outcomes were similar betweenthe groups. In a further analysis Setti et al. (2011), only244 oligoasthenozoospermic patients were included and apositive influence of IMSI on fertilization (OR 4.3, 95% CI2.2–6.4), implantation (OR 2.6, 95% CI 1.2–5.7) and preg-nancy (OR 1.6, 95% CI 1.1–3.0) was observed.
Wilding et al. (2011) randomized 232 couples undergoing ICSIas a result of male factor infertility into ICSI and IMSI groups,and the outcomes were compared. The results showed thatimplantation and pregnancy rates were significantly higher inIMSI group (14.8% versus 24.2% and 40.0% versus 65.6%).
In a recent prospective randomized trial, Knez et al.(2012) compared the outcomes obtained with ICSI (n = 70)and IMSI (n = 52) in couples with isolated teratozoospermia.The study showed a significantly higher rate of morulaedevelopment (21.0% versus 13.0%) and a lower number ofembryos arrested at low-cell developmental stages (44.0%versus 62.0%) after IMSI. A significantly higher clinical preg-nancy rate was observed in the IMSI group compared withthe ICSI group (48.0% versus 24.0%; P < 0.05). In addition,the authors investigated the influence of individual spermmorphology on embryo development in 30 patients undergo-ing IMSI. Oocytes were injected with different classes ofspermatozoa and the results showed that fertilization withspermatozoa without head vacuoles yielded a higher num-ber of morphologically normal zygotes, a higher blastocystformation rate and a smaller proportion of arrested embryosthan spermatozoa with vacuoles and other head defects.
IMSI in unselected infertile patients
Balaban et al. (2011) compared the outcomes of 87 IMSIcycles with 81 ICSI cycles in an unselected infertile popula-tion in a prospective randomized study. The results showedtrends for higher rates of implantation (28.9% versus 19.5%),pregnancy (54.0% versus 44.4%) and live birth (43.7% versus38.3%) in the IMSI group. When only couples presentingsevere male factor were analysed, the IMSI procedureresulted in significantly higher implantation rates comparedwith the ICSI group (29.6% versus 15.2%, P = 0.01).
IMSI in patients with a high rate of sperm DNAfragmentation
Hazout et al. (2006), in a previously mentioned study,assessed sperm DNA integrity in 72 patients. Improvedimplantation and birth rates were observed not only inpatients with an elevated degree of sperm DNA fragmenta-tion but also in those with normal sperm DNA status.
In a previously mentioned study, de Almeida FerreiraBraga et al. (2011) showed that fertilization and high qualityembryo rates in patients with a high incidence of sperm DNAfragmentation were similar between sibling oocytes splitinto ICSI and IMSI groups.
All the aforementioned studies comparing ICSI and IMSIoutcomes are summarized in Table 2.
IMSI in patients with poor blastocyst development
Because early paternal effects on embryo development arenot expressed up to day 3, it has been suggested that the
presenceof nuclear vacuoles, detected under highmagnifica-tion may influence the development to the blastocyst stage.
Vanderzwalmen et al. (2008) investigated the associationbetween the presence of vacuoles in sperm nuclei and theability of embryos to develop to blastocyst stage on day 5of development in couples in which the woman was<40 years old and at least eight oocytes were retrieved.The authors graded spermatozoa from 25 patients as fol-lows: grade I, no vacuoles; grade II, �2 small vacuoles;grade III, �1 large vacuole; and grade IV, large vacuoleswith other morphological abnormalities. The study showedthat after sibling oocyte injection, no differences wereobserved in embryo quality on day 3 of development inthe four different grades of spermatozoa. However, blasto-cyst formation occurred in 56.3% and 61.4% with grade I andII spermatozoa, respectively, compared with 5.1% and 0%with grade III and IV spermatozoa, respectively (P < 0.001).Similarly, Cassuto et al. (2009) showed that only one embryo(5.3%) developed to blastocyst stage after the injection of19 oocytes with score 0 spermatozoa (spermatozoa present-ing several head abnormalities). In addition, Knez et al.(2011) observed a higher number of blastocysts with IMSIas compared with ICSI. In addition, with IMSI 26.0% ofembryos developed to the blastocyst stage after IMSI,whereas in the previous ICSI cycles all embryos werearrested at earlier developmental stages.
De Vos et al. (2013) conducted a prospective randomizedsibling-oocyte study, enrolling 340 couples undergoing ICSIas a result of oligoasthenoteratozoospermia, in order to eval-uate the influence of high-magnification sperm analysis onembryo development. No significant differences wereobserved between ICSI and IMSI for embryo development onday 3 and 5. Despite the low number of grade III and IV sper-matozoa used for injection, it seems that blastocyst forma-tion is not excluded when using these grades of spermatozoa.
IMSI with vacuolated versus non-vacuolated spermatozoa
Berkovitz et al. (2005) investigated whether the higher rateof pregnancy was attributable to the fine nuclear morphol-ogy of the injected spermatozoa by comparing two matchedIMSI groups in which the woman was <40 years old and atleast three oocytes were retrieved. In one group, no sper-matozoa with intact nuclei were available for microinjec-tion, and in the other, only spermatozoa with strictlydefined morphologically normal nuclei were injected. Theresults showed that the fertilization rate (71.3% versus50.3%), percentage of top-quality embryos (34.9% versus19.4%), implantation (25.0% versus 5.9%) and pregnancyrates (52.6% versus 18.4%) were significantly higher, andabortion rates (10.0% versus 57.1%) significantly lower, inthe group in which only spermatozoa with morphologicallynormal nuclei were injected.
In a retrospective study dealing with spermatozoa andspermatids from 11 normozoospermic, 10 oligozoospermicor asthenozoospermic, four obstructive azoospermic andthree nonobstructive azoospermic men, Tanaka et al.(2012) evaluated whether sperm vacuoles affected ICSI out-comes. The results demonstrated that >85% of the cellspossessed vacuoles of various sizes and that this frequencywas significantly higher in ejaculated cells. In addition,removal of the acrosome did not influence sperm vacuoliza-tion. There was no difference in the fertilization rate when
348 AS Setti et al.

spermatozoa with large or small vacuoles and spermatozoawith no vacuoles were injected. However, a significantlylower rate of development to the blastocyst stage wasobserved when spermatozoa with no vacuoles was injected.
IMSI and preimplantation genetic screening (PGS)
Figueira Rde et al. (2011) examined the effect of sperm mor-phology under high magnification on embryo chromosomalstatus in 30 ICSI–PGS and 30 IMSI–PGS cycles performed incouples of advanced maternal age in a prospective random-ized trial. Biological and clinical outcomes were compared.The data showed a significantly increased incidence of sexchromosome aneuploidy in ICSI embryos compared with IMSIembryos (23.5% versus 15.0%, respectively), and the inci-dence of chaotic embryos was also significantly higher underthe ICSI procedure (27.5% versus 18.8%). In addition, the pro-portion of cycles without embryo transfer was significantlyhigher in ICSI–PGS cycles (11.8% versus 2.5%). Furthermore,the authors reported an unexpected significant differencein gender incidence rates of euploid embryos. ‘Best looking’spermatozoa seemed to carry a higher proportion of the Xchromosome. In a recent study performed by the same group,Setti et al. (2012) confirmed the aforementioned finding,showing a significantly higher incidence of XX embryosderived from IMSI compared with ICSI cycles (66.9% versus52.5%, respectively). It is noteworthy that the study evalu-ated the gender of all embryos that were biopsied and didnot consider which of these embryos were transferred,implanted and resulted in live births.
IMSI with testicular spermatozoa
Ai et al. (2010) investigated whether IMSI with testicularspermatozoa improves the clinical outcome in patients withazoospermia. A total of 66 azoospermic patients were pro-vided with conventional ICSI and 39 with IMSI. The resultsshowed no difference between groups regarding pregnancyrates; however, the rate of early abortion was significantlylower in the IMSI group compared with the ICSI group (4.5%and 11.8%, respectively).
IMSI in patients with globozoospermia andmacrocephalic sperm head syndrome
The high magnification approach is also of particular benefitwhen used in situations in which the identification of spe-cific sperm organelles is required, such as the acrosomalcomponents in cases of globozoospermia. Sermondadeet al. (2011) reported a successful pregnancy and healthychildbirth in a case of total globozoospermia after IMSI.
Chelli et al. (2010) studied the chromosomal content ofspermatozoa selected by IMSI in two cases of macrocephalicsperm head syndrome. FISH was performed in selected sper-matozoa with normal-sized heads after IMSI selection. How-ever, of the six spermatozoa that could be selected, allwere aneuploid.
IMSI drawbacks
Sperm selection under high magnification is performed usinga glass-bottomed dish that is appropriate for Nomarski
microscopy. On the other hand, the ICSI procedure is per-formed with a plastic-bottomed dish that works with Hoff-man modulation contrast. Therefore, it is important toemphasize that switching between the two systems requiresadditional time, delaying the injection procedure.
In addition, high magnification requires the use of anappropriate video camera and software system, which isable to provide digital zoom, an aspect that make MSOMEand IMSI very expensive approaches. It is noteworthy thatfor IMSI, the optical magnification uses ranges from ·1000to ·1500 and the additional magnification (·6600 and soon) involves digital magnification with no further gain inresolution.
Berkovitz et al. (2005) mentioned that the selection pro-cess has an average range of duration between 1.5–5 h.Indeed, Balaban et al. (2011) demonstrated that the dura-tion of the procedure was significantly longer in the IMSIgroup as compared with the ICSI group (13.6 min versus20.5 min; P < 0.001). Having said that, the extra time nec-essary for sperm selection and the elevated equipmentcosts are a limitation to a more widespread use of IMSI.
To date, a single study reported a potential harmfulimpact of IMSI on the outcomes (Junca et al., 2010). A sig-nificantly higher incidence of low birthweights for IMSIinfants was observed as compared with ICSI (29.1% versus23.1%).
Conclusions
Sperm selection methods are an important challenge inassisted reproduction because most sperm characteristicscannot be tested, either in real time or in single cellsreferred to the ICSI procedure. Sperm selection under amagnification of ·400, in preparation for ICSI, allows theidentification of major sperm morphological defects butdoes not provide information regarding the nuclear statusof the sperm cell.
An interesting solution was introduced with the advent ofMSOME, which is performed prior to the IMSI procedure,under an overall optical magnification of at least ·6000,enabling the selection of spermatozoa free of nuclearvacuoles, which are related to blockage of embryonicdevelopment during and/or after implantation. Therefore,IMSI has been proposed as an alternative to routine ICSI,initially for couples with repeated ICSI failures and subse-quently for couples with increased rates of DNA-fragmentedspermatozoa.
The efficiency of IMSI with regard to subsequent fertiliza-tion, embryo development, implantation, pregnancy andmiscarriage rates has been the focus of several studies;however, the results are controversial. These conflictingresults might have occurred due to differences in inclusioncriteria, stimulation protocols, seminal and oocyte qualitiesand many other confounding variables within the IVF cycles.
In general, studies have not observed significant differ-ences in fertilization rate following ICSI and IMSI. It has beensuggested that IMSI is not beneficial at improving the earlypaternal effects (Mauri et al., 2010). Clinical evidence fromassisted reproduction suggests that failure to complete thefertilization process, syngamy or early cleavage might bethe result of an early paternal effect (Barroso et al., 2009).
MSOME and IMSI: a review 349

This phenomenon may also account for the similar resultsobtained with embryo quality after ICSI and IMSI. Anotherimportant fact that could have influenced this outcome isthe day of development at which the top-quality embryorate was calculated.
On the other hand, the late paternal effect is character-ized by poor embryo development to blastocyst stage,implantation failure and pregnancy loss and is associatedwith sperm abnormalities at the level of DNA chromatin.Despite some controversies, several studies observed ten-dencies or significantly better outcomes, mainly in blasto-cyst formation, pregnancy and implantation rates,following the utilization of IMSI compared with conventionalICSI. Therefore, it seems that IMSI is effective in overcomingthe late paternal effects.
In the light of these findings, MSOME seems to be a surro-gate tool for the selection of strictly morphologically nor-mal spermatozoa prior to oocyte injection, resulting inhigher rates of embryonic development, blastocyst forma-tion, implantation and pregnancy. It is noteworthy thatmore prospective randomized trials are required to confirmthe superiority of IMSI over conventional ICSI and to identifythe causes of infertility that could benefit from the IMSI pro-cedure. Nevertheless, as Vanderzwalmen and Fallet (2010)proposed: ‘Are there any indications to not select the bestspermatozoa? Of course not.’
References
Ai, L., Liu, S.Y., Huang, J., Chen, S.W., Liu, J., Zhong, Y., 2010.Intracytoplasmic morphologically selected sperm injection oftesticular sperm: clinical outcome in azoospermia patients.Zhonghua Nan Ke Xue 16, 826–829.
Antinori, M., Licata, E., Dani, G., Cerusico, F., Versaci, C.,D’Angelo, D., Antinori, S., 2008. Intracytoplasmic morphologi-cally selected sperm injection: a prospective randomized trial.Reprod. Biomed. Online 16, 835–841.
Baccetti, B., Collodel, G., Piomboni, P., 1996. Apoptosis in humanejaculated sperm cells (notulae seminologicae 9). J. Submi-crosc. Cytol. Pathol. 28, 587–596.
Balaban, B., Yakin, K., Alatas, C., Oktem, O., Isiklar, A., Urman, B.,2011. Clinical outcome of intracytoplasmic injection of sperma-tozoa morphologically selected under high magnification: aprospective randomized study. Reprod. Biomed. Online 22,472–476.
Barroso, G., Valdespin, C., Vega, E., Kershenovich, R., Avila, R.,Avendano, C., Oehninger, S., 2009. Developmental spermcontributions: fertilization and beyond. Fertil. Steril. 92,835–848.
Bartoov, B., Berkovitz, A., Eltes, F., 2001. Selection of spermatozoawith normal nuclei to improve the pregnancy rate with intracy-toplasmic sperm injection. N. Engl. J. Med. 345, 1067–1068.
Bartoov, B., Berkovitz, A., Eltes, F., Kogosowski, A., Menezo, Y.,Barak, Y., 2002. Real-time fine morphology of motile humansperm cells is associated with IVF-ICSI outcome. J. Androl. 23,1–8.
Bartoov, B., Berkovitz, A., Eltes, F., Kogosovsky, A., Yagoda, A.,Lederman, H., Artzi, S., Gross, M., Barak, Y., 2003. Pregnancyrates are higher with intracytoplasmic morphologically selectedsperm injection than with conventional intracytoplasmic injec-tion. Fertil. Steril. 80, 1413–1419.
Berkovitz, A., Eltes, F., Soffer, Y., Zabludovsky, N., Beyth, Y.,Farhi, J., Levran, D., Bartoov, B., 1999. ART success and in vivosperm cell selection depend on the ultramorphological status ofspermatozoa. Andrologia 31, 1–8.
Berkovitz, A., Eltes, F., Yaari, S., Katz, N., Barr, I., Fishman, A.,Bartoov, B., 2005. The morphological normalcy of the spermnucleus and pregnancy rate of intracytoplasmic injection withmorphologically selected sperm. Hum. Reprod. 20, 185–190.
Berkovitz, A., Eltes, F., Ellenbogen, A., Peer, S., Feldberg, D.,Bartoov, B., 2006a. Does the presence of nuclear vacuoles inhuman sperm selected for ICSI affect pregnancy outcome? Hum.Reprod. 21, 1787–1790.
Berkovitz, A., Eltes, F., Lederman, H., Peer, S., Ellenbogen, A.,Feldberg, B., Bartoov, B., 2006b. How to improve IVF-ICSIoutcome by sperm selection. Reprod. Biomed. Online 12,634–638.
Boitrelle, F., Ferfouri, F., Petit, J.M., Segretain, D., Tourain, C.,Bergere, M., Bailly, M., Vialard, F., Albert, M., Selva, J., 2011.Large human sperm vacuoles observed in motile spermatozoaunder high magnification: nuclear thumbprints linked to failureof chromatin condensation. Hum. Reprod. 26, 1650–1658.
Boitrelle, F., Albert, M., Theillac, C., Ferfouri, F., Bergere, M.,Vialard, F., Wainer, R., Bailly, M., Selva, J., 2012. Cryopreser-vation of human spermatozoa decreases the number of motilenormal spermatozoa, induces nuclear vacuolization and chro-matin decondensation. J. Androl. 33, 1371–1378.
Borini, A., Tarozzi, N., Bizzaro, D., Bonu, M.A., Fava, L., Flamigni,C., Coticchio, G., 2006. Sperm DNA fragmentation: paternaleffect on early post-implantation embryo development in ART.Hum. Reprod. 21, 2876–2881.
Braude, P., Bolton, V., Moore, S., 1988. Human gene expressionfirst occurs between the four- and eight-cell stages of preim-plantation development. Nature 332, 459–461.
Calamera, J.C., Fernandez, P.J., Buffone, M.G., Acosta, A.A.,Doncel, G.F., 2001. Effects of long-term in vitro incubation ofhuman spermatozoa: functional parameters and catalase effect.Andrologia 33, 79–86.
Cassuto, N.G., Bouret, D., Plouchart, J.M., Jellad, S., Vanderzwal-men, P., Balet, R., Larue, L., Barak, Y., 2009. A new real-timemorphology classification for human spermatozoa: a link forfertilization and improved embryo quality. Fertil. Steril. 92,1616–1625.
Cassuto, N.G., Hazout, A., Hammoud, I., Balet, R., Bouret, D.,Barak, Y., Jellad, S., Plouchart, J.M., Selva, J., Yazbeck, C.,2012. Correlation between DNA defect and sperm-head mor-phology. Reprod. Biomed. Online 24, 211–218.
Chelli, M.H., Albert, M., Ray, P.F., Guthauser, B., Izard, V.,Hammoud, I., Selva, J., Vialard, F., 2010. Can intracytoplasmicmorphologically selected sperm injection be used toselect normal-sized sperm heads in infertile patients withmacrocephalic sperm head syndrome? Fertil. Steril. 93,e1341–1345.
Chrzanowski, S., 1966. Ultrastructure of human spermatozoon. Pol.Med. J. 5, 482–491.
de Almeida Ferreira Braga, D.P., Setti, A.S., Figueira, R.C., Nichi,M., Martinhago, C.D., Iaconelli Jr., A., Borges Jr., E., 2011.Sperm organelle morphologic abnormalities: contributing fac-tors and effects on intracytoplasmic sperm injection cyclesoutcomes. Urology 78, 786–791.
De Vos, A., Van de Velde, H., Bocken, G., Eylenbosch, G., Franceus,N., Meersdom, G., Tistaert, S., Vankelecom, A., Tournaye, H.,Verheyen, G., 2013. Does intracytoplasmic morphologicallyselected sperm injection improve embryo development? Arandomized sibling-oocyte study. Hum. Reprod. 28, 617–626.
Fawcett, D., 1958. The structure of the mammalian spermatozoon.Int. Rev. Cytol. 7, 195–234.
Figueira Rde, C., Braga, D.P., Setti, A.S., Iaconelli Jr., A., BorgesJr., E., 2011. Morphological nuclear integrity of sperm cells isassociated with preimplantation genetic aneuploidy screeningcycle outcomes. Fertil. Steril. 95, 990–993.
Franco Jr., J.G., Baruffi, R.L., Mauri, A.L., Petersen, C.G., Oliveira,J.B., Vagnini, L., 2008. Significance of large nuclear vacuoles in
350 AS Setti et al.
human spermatozoa: implications for ICSI. Reprod. Biomed.Online 17, 42–45.
Franco Jr., J.G., Mauri, A.L., Petersen, C.G., Massaro, F.C., Silva,L.F., Felipe, V., Cavagna, M., Pontes, A., Baruffi, R.L., Oliveira,J.B., Vagnini, L.D., 2012. Large nuclear vacuoles are indicativeof abnormal chromatin packaging in human spermatozoa. Int. J.Androl. 35, 46–51.
Garolla, A., Fortini, D., Menegazzo, M., De Toni, L., Nicoletti, V.,Moretti, A., Selice, R., Engl, B., Foresta, C., 2008. High-powermicroscopy for selecting spermatozoa for ICSI by physiologicalstatus. Reprod. Biomed. Online 17, 610–616.
Gonzalez-Ortega, C., Cancino-Villarreal, P., Perez-Torres, A.,Vargas-Maciel, M.A., Martinez-Garza, S.G., Perez-Pena, E.,Gutierrez-Gutiedrrez, A.M., 2010. Intracytoplasmic morpholog-ically selected sperm injection (IMSI) vs intracytoplasmic sperminjection (ICSI) in patients with repeated ICSI failure. Ginecol.Obstet. Mex. 78, 652–659.
Hammoud, I., Boitrelle, F., Ferfouri, F., Vialard, F., Bergere, M.,Wainer, B., Bailly, M., Albert, M., Selva, J., 2013. Selection ofnormal spermatozoa with a vacuole-free head (·6300) improvesselection of spermatozoa with intact DNA in patients with highsperm DNA fragmentation rates. Andrologia 45, 163–170.
Hazout, A., Dumont-Hassan, M., Junca, A.M., Cohen Bacrie, P.,Tesarik, J., 2006. High-magnification ICSI overcomes paternaleffect resistant to conventional ICSI. Reprod. Biomed. Online 12,19–25.
Host, E., Ernst, E., Lindenberg, S., Smidt-Jensen, S., 2001.Morphology of spermatozoa used in IVF and ICSI from oligozoo-spermic men. Reprod. Biomed. Online 3, 212–215.
Junca, A.M., Dumont, M., Cornet, D., Douard, S., De Mouzon, J.,Prisant, N., 2010. Is intracytoplasmic morphologically selectedsperm injection (IMSI) detrimental for pregnancy outcome?Fertil. Steril. 94, S31.
Kacem, O., Sifer, C., Barraud-Lange, V., Ducot, B., De Ziegler, D.,Poirot, C., Wolf, J., 2011. Sperm nuclear vacuoles, as assessedby motile sperm organellar morphological examination, aremostly of acrosomal origin. Reprod. Biomed. Online 20,132–137.
Knez, K., Zorn, B., Tomazevic, T., Vrtacnik-Bokal, E., Virant-Klun,I., 2011. The IMSI procedure improves poor embryo developmentin the same infertile couples with poor semen quality: acomparative prospective randomized study. Reprod. Biol. Endo-crinol. 9, 123.
Knez, K., Tomazevic, T., Zorn, B., Vrtacnik-Bokal, E., Virant-Klun,I., 2012. Intracytoplasmic morphologically selected sperminjection improves development and quality of preimplantationembryos in teratozoospermia patients. Reprod. Biomed. Online25, 168–179.
Kruger, T.F., Menkveld, R., Stander, F.S., Lombard, C.J., Van derMerwe, J.P., van Zyl, J.A., Smith, K., 1986. Sperm morphologicfeatures as a prognostic factor in in vitro fertilization. Fertil.Steril. 46, 1118–1123.
Kruger, T.F., Acosta, A.A., Simmons, K.F., Swanson, R.J., Matta,J.F., Veeck, L.L., Morshedi, M., Brugo, S., 1987. New method ofevaluating sperm morphology with predictive value for humanin vitro fertilization. Urology 30, 248–251.
Kruger, T.F., Acosta, A.A., Simmons, K.F., Swanson, R.J., Matta,J.F., Oehninger, S., 1988. Predictive value of abnormal spermmorphology in in vitro fertilization. Fertil. Steril. 49, 112–117.
Mauri, A.L., Petersen, C.G., Oliveira, J.B., Massaro, F.C., Baruffi,R.L., Franco Jr., J.G., 2010. Comparison of day 2 embryo qualityafter conventional ICSI versus intracytoplasmic morphologicallyselected sperm injection (IMSI) using sibling oocytes. Eur. J.Obstet. Gynecol. Reprod. Biol. 150, 42–46.
Monqaut, A.L., Zavaleta, C., Lopez, G., Lafuente, R., Brassesco,M., 2011. Use of high-magnification microscopy for the assess-ment of sperm recovered after two different sperm processingmethods. Fertil. Steril. 95, 277–280.
Montjean, D., Belloc, S., Benkhalifa, M., Dalleac, A., Menezo, Y.,2012. Sperm vacuoles are linked to capacitation and acrosomalstatus. Hum. Reprod. 27, 2927–2932.
Morozumi, K., Yanagimachi, R., 2005. Incorporation of the acro-some into the oocyte during intracytoplasmic sperm injectioncould be potentially hazardous to embryo development. Proc.Natl. Acad. Sci. U.S.A. 102, 14209–14214.
Mundy, A.J., Ryder, T.A., Edmonds, D.K., 1994. A quantitativestudy of sperm head ultrastructure in subfertile males withexcess sperm precursors. Fertil. Steril. 61, 751–754.
Nagy, Z.P., Verheyen, G., Tournaye, H., Van Steirteghem, A.C.,1998. Special applications of intracytoplasmic sperm injection:the influence of sperm count, motility, morphology, source andsperm antibody on the outcome of ICSI. Hum. Reprod. 13,143–154.
O’Connell, M., McClure, N., Lewis, S.E., 2002. The effects ofcryopreservation on sperm morphology, motility and mitochon-drial function. Hum. Reprod. 17, 704–709.
Oehninger, S., Chaturvedi, S., Toner, J., Morshedi, M., Mayer, J.,Lanzendorf, S., Muasher, S., 1998. Semen quality: is there apaternal effect on pregnancy outcome in in-vitro fertiliza-tion/intracytoplasmic sperm injection? Hum. Reprod. 13,2161–2164.
Oliveira, J.B., Massaro, F.C., Mauri, A.L., Petersen, C.G., Nicoletti,A.P., Baruffi, R.L., Franco Jr., J.G., 2009. Motile spermorganelle morphology examination is stricter than Tygerbergcriteria. Reprod. Biomed. Online 18, 320–326.
Oliveira, J.B., Massaro, F.C., Baruffi, R.L., Mauri, A.L., Petersen,C.G., Silva, L.F., Vagnini, L.D., Franco Jr., J.G., 2010a.Correlation between semen analysis by motile sperm organellemorphology examination and sperm DNA damage. Fertil. Steril.94, 1937–1940.
Oliveira, J.B., Petersen, C.G., Massaro, F.C., Baruffi, R.L., Mauri,A.L., Silva, L.F., Ricci, J., Franco Jr., J.G., 2010b. Motile spermorganelle morphology examination (MSOME): intervariationstudy of normal sperm and sperm with large nuclear vacuoles.Reprod. Biol. Endocrinol. 8, 56.
Oliveira, J.B., Cavagna, M., Petersen, C.G., Mauri, A.L., Massaro,F.C., Silva, L.F., Baruffi, R.L., Franco Jr., J.G., 2011. Pregnancyoutcomes in women with repeated implantation failures afterintracytoplasmic morphologically selected sperm injection(IMSI). Reprod. Biol. Endocrinol. 9, 99.
Palermo, G., Joris, H., Devroey, P., Van Steirteghem, A.C., 1992.Pregnancies after intracytoplasmic injection of single sperma-tozoon into an oocyte. Lancet 340, 17–18.
Pedersen, H., 1969. Ultrastructure of the ejaculated human sperm.Z. Zellforsch. Mikrosk. Anat. 94, 542–554.
Peer, S., Eltes, F., Berkovitz, A., Yehuda, R., Itsykson, P., Bartoov,B., 2007. Is fine morphology of the human sperm nuclei affectedby in vitro incubation at 37 degrees C? Fertil. Steril. 88,1589–1594.
Perdrix, A., Travers, A., Chelli, M.H., Escalier, D., Do Rego, J.L.,Milazzo, J.P., Mousset-Simeon, N., Mace, B., Rives, N., 2011.Assessment of acrosome and nuclear abnormalities inhuman spermatozoa with large vacuoles. Hum. Reprod. 26,47–58.
Perdrix, A., Saidi, R., Menard, J.F., Gruel, E., Milazzo, J.P., Mace,B., Rives, N., 2012. Relationship between conventional spermparameters and motile sperm organelle morphology examination(MSOME). Int. J. Androl. 35, 491–498.
Ruzin, S.E., 1999. Plant microtechnique and microscopy, first ed.Oxford University Press, New York.
Said, T.M., Land, J.A., 2011. Effects of advanced selection methodson sperm quality and ART outcome: a systematic review. Hum.Reprod. Update 17, 719–733.
Schultz-Larsen, J., 1958. The morphology of the human sperm;electron microscopic investigations of the ultrastructure. ActaPathol. Microbiol. Scand. Suppl. 44, 1–121.
MSOME and IMSI: a review 351

Sermondade, N., Hafhouf, E., Dupont, C., Bechoua, S., Palacios, C.,Eustache, F., Poncelet, C., Benzacken, B., Levy, R., Sifer, C.,2011. Successful childbirth after intracytoplasmic morphologi-cally selected sperm injection without assisted oocyte activationin a patient with globozoospermia. Hum. Reprod. 26,2944–2949.
Setti, A.S., Figueira, R.D., Braga, D.P., Iaconelli Jr., A., Borges Jr.,E., 2011. Intracytoplasmic morphologically selected sperminjection benefits for patients with oligoasthenozoospermiaaccording to the 2010 World Health Organization referencevalues. Fertil. Steril. 95, 2711–2714.
Setti, A.S., Figueira, R.C., Braga, D.P., Iaconelli Jr., A., Borges Jr.,E., 2012. Gender incidence of intracytoplasmic morphologicallyselected sperm injection-derived embryos: a prospective ran-domized study. Reprod. Biomed. Online 24, 420–423.
Silva, L.F., Oliveira, J.B., Petersen, C.G., Mauri, A.L., Massaro,F.C., Cavagna, M., Baruffi, R.L., Franco Jr., J.G., 2012. Theeffects of male age on sperm analysis by motile sperm organellemorphology examination (MSOME). Reprod. Biol. Endocrinol. 10,19.
Souza Setti, A., Ferreira, R.C., Paes de Almeida Ferreira Braga, D.,de Cassia Savio Figueira, R., Iaconelli Jr., A., Borges Jr., E.,2010. Intracytoplasmic sperm injection outcome versusintracytoplasmic morphologically selected sperm injectionoutcome: a meta-analysis. Reprod. Biomed. Online 21,450–455.
Tanaka, A., Nagayoshi, M., Tanaka, I., Kusunoki, H., 2012. Humansperm head vacuoles are physiological structures formed duringthe sperm development and maturation process. Fertil. Steril.98, 315–320.
Tesarik, J., Greco, E., Mendoza, C., 2004. Late, but not early,paternal effect on human embryo development is related tosperm DNA fragmentation. Hum. Reprod. 19, 611–615.
Vanderzwalmen, P., Fallet, C., 2010. IMSI: indications, results andreflexions. J. Gynecol. Obstet. Biol. Reprod. (Paris) 39, 22–25.
Vanderzwalmen, P., Hiemer, A., Rubner, P., Bach, M., Neyer, A.,Stecher, A., Uher, P., Zintz, M., Lejeune, B., Vanderzwalmen, S.,Cassuto, G., Zech, N.H., 2008. Blastocyst development after spermselection at highmagnification is associatedwith size and number ofnuclear vacuoles. Reprod. Biomed. Online 17, 617–627.
Watanabe, S., Tanaka, A., Fujii, S., Mizunuma, H., Fukui, A.,Fukuhara, R., Nakamura, R., Yamada, K., Tanaka, I., Awata, S.,Nagayoshi, M., 2011. An investigation of the potential effect ofvacuoles in human sperm on DNA damage using a chromosomeassay and the TUNEL assay. Hum. Reprod. 26, 978–986.
WHO, 1999. WHO laboratory manual for the examination of humansemen and sperm-cervical mucus interaction, fourth ed. Pub-lished on behalf of the World Health Organization by CambridgeUniversity Press, Cambridge, UK.
Wilding, M., Coppola, G., di Matteo, L., Palagiano, A., Fusco, E.,Dale, B., 2011. Intracytoplasmic injection of morphologicallyselected spermatozoa (IMSI) improves outcome after assistedreproduction by deselecting physiologically poor quality sper-matozoa. J. Assist. Reprod. Genet. 28, 253–262.
Declaration: The authors report no financial or commercialconflicts of interest.
Received 16 August 2012; refereed 19 June 2013; accepted 19 June2013.
352 AS Setti et al.

Review
Intracytoplasmic morphologically selected sperm injection resultsin improved clinical outcomes in couples with previous ICSI failuresor male factor infertility: a meta-analysis
Amanda S. Setti a,b,c, Daniela P.A.F. Braga a,b, Rita C.S. Figueira b,c, Assumpto Iaconelli Jr.a,b,Dr.Edson Borges a,b,*a Instituto Sapientiae—Centro de Estudos e Pesquisa em Reproducao Assistida, Rua Vieira Maciel, 62, Sao Paulo 04503-040, SP, Brazilb Fertility—Centro de Fertilizacao Assistida, Av. Brigadeiro Luis Antonio, 4545, Sao Paulo 01401-002, SP, Brazilc Faculdade de Ciencias Medicas da Santa Casa de Sao Paulo, Rua Dr. Cesario Motta Junior, 61, Sao Paulo 01221-020, SP, Brazil
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Literature search . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Study selection and data extraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Statistical analysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Literature identification and study characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Data on ICSI outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Couples with previous implantation failures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Implantation rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Pregnancy rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Miscarriage rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
European Journal of Obstetrics & Gynecology and Reproductive Biology 183 (2014) 96–103
A R T I C L E I N F O
Article history:
Received 19 May 2014
Received in revised form 6 August 2014
Accepted 4 October 2014
Keywords:
Implantation
IMSI
Male factor
Miscarriage
MSOME
Sperm morphology
A B S T R A C T
The objective of this study was to perform the first meta-analysis to compare conventional
intracytoplasmic sperm injection (ICSI) outcomes and intracytoplasmic morphologically selected
sperm injection (IMSI) outcomes in couples with previous ICSI failures (IF) or male factor infertility
(MF). A systematic review was performed by searching Medline database to identify articles reporting
on the comparison between ICSI and IMSI outcomes in couples with IF or MF. The main outcome
measures were the implantation, pregnancy and miscarriage rates. Thirteen studies fulfilled our
predetermined criteria. The overall results of meta-analysis for implantation (OR: 2.88; CI: 2.13–
3.89), pregnancy (OR: 2.07; CI: 1.22–3.50) and miscarriage rates (OR: 0.31; CI: 0.14–0.67) were in
favor of IMSI in couples with IF. Additionally, the overall result of meta-analysis for implantation (OR:
1.56; CI: 1.11–2.18) and pregnancy rate (OR: 1.61; CI: 1.17–2.23) were in favor of IMSI in couples with
MF. IMSI increases the odds of implantation by 50% and pregnancy by 60% in couples with MF. In light
of improved clinical outcomes, we recommend promoting the IMSI method in couples with MF.
Moreover, IMSI results in a 3-fold increase in implantation rate, a 2-fold increase in pregnancy rate
and a 70% decrease in miscarriage rate as compared to ICSI in couples with IF, however, as no
randomized evidence exists, randomized studies are needed to confirm the IMSI benefits in couples
with IF.
� 2014 Elsevier Ireland Ltd. All rights reserved.
* Corresponding author at: Fertility—Centro de Fertilizacao Assistida, Clinical Director, Av. Brigadeiro Luis Antonio, 4545, Sao Paulo 01401-002, SP, Brazil.
Tel.: +55 11 3018 8181; fax: +55 11 30188182.
E-mail address: [email protected] (E. Borges).
Contents lists available at ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
jou r nal h o mep ag e: w ww .e lsev ier . co m / loc ate /e jo g rb
http://dx.doi.org/10.1016/j.ejogrb.2014.10.008
0301-2115/� 2014 Elsevier Ireland Ltd. All rights reserved.

Couples with male factor infertility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Implantation rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Pregnancy rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Miscarriage rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Comment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Condensation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Introduction
In the last decade a new approach involving real-time, high-magnification observation of unstained spermatozoa, named‘motile sperm organelle morphology examination’ (MSOME),has been introduced [1]. The incorporation of this techniquetogether with a micromanipulation system has allowed theintroduction of a modified intracytoplasmic sperm injection(ICSI) procedure, known as intracytoplasmic morphologicallyselected sperm injection (IMSI). This system of real-timedetailed morphological sperm examination at high magnifica-tion, ranging from �6600 to �13,000 with Nomarski optics,enables the selection of the best available motile spermatozoabefore oocyte injection [2–5].
Several studies have investigated the benefits of IMSI bycomparing the results obtained using this technique with thoseobtained via ICSI; however, the results are controversial [2–18]. Nevertheless, numerous publications have reported that IMSIis positively associated with implantation and/or pregnancy rates[2–5,7–12,16–18] in couples with previous and repeated implan-tation failures and in patients with male factor infertility.
Meta-analysis provides an overall consensus from studies,resulting in a more precise estimate than any of the individualarticles. A meta-analysis, published in 2010, comparing ICSI vs.IMSI outcomes concluded that IMSI not only significantly improvesthe percentage of top-quality embryos, implantation and preg-nancy rates, but also significantly reduces miscarriage rates ascompared with ICSI [19]. However, this previous meta-analysisincluded a single randomized controlled trial and two non-randomized studies. Similarly, a more recent meta-analysisshowed a very-low-quality evidence that IMSI improves clinicalpregnancy [20]. These two meta-analyses did not take into accountthe indications for ICSI; therefore, their results cannot begeneralized for all the couples undergoing ICSI. Therefore, theaim of this study was to perform the first meta-analysis to compareconventional intracytoplasmic sperm injection (ICSI) outcomesand intracytoplasmic morphologically selected sperm injection(IMSI) outcomes in couples with previous ICSI failures (IF) or malefactor infertility (MF).
Materials and methods
Literature search
A computerized search in MEDLINE (from January 2001 untilApril 2013) was performed to identify articles reporting onthe comparison between ICSI and IMSI outcomes. Keywords usedwere: ‘‘Intracytoplasmic morphologically selected sperm injec-tion’’, ‘‘motile sperm organelle morphology examination’’ ‘‘IMSI’’,‘‘MSOME’’ and ‘‘high magnification ICSI’’. The search was notrestricted for articles written in English. References detected withthe related articles function in Pubmed were also checked toidentify cited articles not captured by electronic searches. Thereference lists of eligible primary studies were examined foridentification of additional articles.
Study selection and data extraction
Grey literature (abstracts, unpublished studies, conferenceproceedings, graduate theses, book chapters, company reports, andapplications) was not included in this meta-analysis. Studiesdealing with azoospermia and sperm DNA fragmentation andstudies in which patients acted as their own controls wereexcluded from the subsequent analysis. No strict selectionaccording to the experimental designs or language was applied.The main outcome measures were implantation, pregnancy andmiscarriage rates. Studies were selected in a two-stage process(illustrated in Fig. 1). At the first screening, the titles and abstractsfrom the electronic searches were scrutinized by two reviewersindependently (A.S. and D.B.). Studies with lack of any relevancewere excluded and full manuscripts of all citations that were likelyto meet the predefined selection criteria were obtained. Second,final inclusion or exclusion decisions were made on examination offull manuscripts by both reviewers.
Two independent investigators (A.S. and D.B.) extracted thedata from all eligible trials. Discrepancies were resolved by theinvolvement of another investigator (R.F.). From each eligible trialwe recorded for both arms the following data: demographic
Fig. 1. Study selection process for systematic review.
A.S. Setti et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 183 (2014) 96–103 97

(authors, type of study, country of origin, patients’ mean age atenrollment and period of enrollment), procedural (number ofpatients included, inclusion and exclusion criteria for patients’populations) and outcome data (implantation, pregnancy andmiscarriage rates).
The Newcastle–Ottawa Quality Assessment Scales for obser-vational studies [21] were implemented. This instrumentassesses the quality of nonrandomized studies in 3 broadcategories (patient selection [4 criteria], comparability of studygroups [1 criterion], and assessment of the outcome [3 criteria]).In this meta-analysis, following quality assessment standards ofprevious meta-analyses, studies that met 5 or more of theNewcastle–Ottawa Scale criteria were considered to be of higherquality.
Statistical analysis
From each study, outcome data were extracted in 2 � 2 tablesby the two reviewers (A.S. and D.B.). The measure of heterogeneity(non-combinability) was evaluated by I2. For a non-significant I2
result a fixed model was used. For a significant I2 result, a randommodel (DerSimonian and Laird) was used. The results were pulledusing Mantel–Haenszel statistic model and are expressed as ORswith 95% confidence intervals (CIs). The meta-analysis wasconducted using the RevMan 5.2 Software (Cochrane Collabora-tion, Oxford, UK).
Results
Literature identification and study characteristics
The process of literature identification and selection issummarized in Fig. 1. A total of 171 studies were initiallyretrieved from the literature. At first screening, after removingduplicates (n = 76) and excluding citations after screeningtitles and/or abstracts (n = 67), a total of 28 published studies,which compared IMSI and ICSI outcomes, were consideredfor inclusion [2–16,18,22–33]. After the second screening,out of the 28 studies, 13 fulfilled our predetermined criteria[2,5–8,10–12,14–16,22,33]. The included studies and theircharacteristics, as well as the results for the Newcastle–Ottawaquality assessment scales for non-randomized studies arelisted in Table 1.
Data on ICSI outcomes
The 13 selected studies comprised 1715 IMSI cycles and2750 ICSI cycles. The quality and the main characteristics of theincluded studies are presented in Table 1. The overall result of themeta-analysis is displayed in Fig. 2.
Couples with previous implantation failures
Out of the thirteen selected studies, six investigated coupleswith previous implantation failures [2,5,7,8,10,14]. The six studiescomprised 440 IMSI cycles and 667 ICSI cycles.
Implantation rate
Four studies reported their implantation rates. A total of 181gestational sacs resulted from 680 transferred embryos (26.6%)in IMSI cycles compared with 76 out of 635 in ICSI cycles (12.0%).The overall result of meta-analysis was in favor of IMSI andconsidered as statistically significant (OR: 2.88; CI: 2.13–3.89)(Fig. 2.1a).
Pregnancy rate
Six studies reported their pregnancy rates. In IMSI group, a totalof 188 pregnancies were obtained out of 440 cycles (47.0%) and189 out of 667 ICSI cycles (28.3%). The overall result of meta-analysis was in favor of IMSI and considered as statisticallysignificant (OR: 2.07; CI: 1.22–3.50) (Fig. 2.1b).
Miscarriage rate
Four studies reported their miscarriage rates. In IMSI cycles, 15miscarriages occurred out of 114 pregnancies (13.2%) comparedwith 19 out of 58 in ICSI cycles (32.8%). The overall result of meta-analysis was in favor of IMSI and considered as statisticallysignificant (OR: 0.31; CI: 0.14–0.67) (Fig. 2.1c).
Couples with male factor infertility
Out of the thirteen selected studies, ten investigated coupleswith male factor infertility [6,7,10–12,14–16,22,33]. The tenstudies comprised 1275 IMSI cycles and 2083 ICSI cycles.
Implantation rate
Seven studies reported their implantation rates. A total of 417gestational sacs resulted from 1908 transferred embryos (21.9%) inIMSI cycles compared with 314 out of 1838 in ICSI cycles (17.1%).The overall result of meta-analysis was in favor of IMSI andconsidered as statistically significant (OR: 1.56; CI: 1.11–2.18)(Fig. 2.2a).
Pregnancy rate
Nine studies reported their pregnancy rates. In IMSI group, atotal of 534 pregnancies were obtained out of 1234 cycles (43.3%)and 782 out of 2029 ICSI cycles (38.5%). The overall result of meta-analysis was in favor of IMSI and considered as statisticallysignificant (OR: 1.61; CI: 1.17–2.23) (Fig. 2.2b).
Miscarriage rate
Six studies reported their miscarriage rates. In IMSI cycles, 53miscarriages occurred out of 369 pregnancies (14.4%) comparedwith 50 out of 289 in ICSI cycles (17.3%). No significant differencewas observed between the IMSI and ICSI groups (OR: 0.86; CI:0.56–1.32) (Fig. 2.2c).
Comment
This is the first meta-analysis that draws together the reports ofthe ICSI � IMSI outcomes, addressing couples with IF or MF. Out of28 relevant studies identified in the current literature, 13 studiesmet the eligibility criteria and were identified as suitable for thismeta-analysis. The overall results of our meta-analysis forimplantation, pregnancy and miscarriage rates were in favor ofIMSI in couples with IF. Additionally, the overall result of our meta-analysis for implantation and pregnancy rate was in favor of IMSIin couples with MF.
It is now well established that the sperm is necessary not onlyfor the key events of fertilization, such as the activation of oocyte,but also for embryonic development from the initial cleavages tothe activation of the embryonic genome. It has been demonstratedthat spermatozoa have an early and a late paternal effect onembryonic development [34]. The early paternal effect caninfluence fertilization and early stages of embryo developmentand is the consequence of sperm cytoplasmic content. The late
A.S. Setti et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 183 (2014) 96–10398
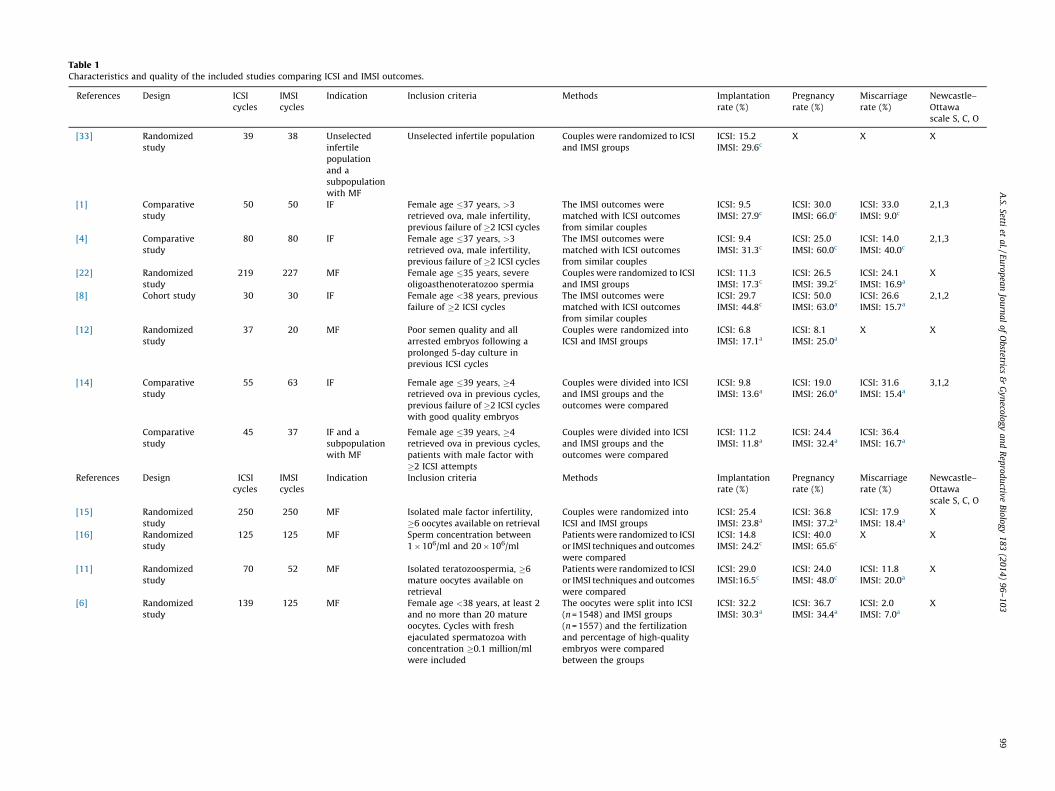
Table 1Characteristics and quality of the included studies comparing ICSI and IMSI outcomes.
References Design ICSI
cycles
IMSI
cycles
Indication Inclusion criteria Methods Implantation
rate (%)
Pregnancy
rate (%)
Miscarriage
rate (%)
Newcastle–
Ottawa
scale S, C, O
[33] Randomized
study
39 38 Unselected
infertile
population
and a
subpopulation
with MF
Unselected infertile population Couples were randomized to ICSI
and IMSI groups
ICSI: 15.2
IMSI: 29.6c
X X X
[1] Comparative
study
50 50 IF Female age �37 years, >3
retrieved ova, male infertility,
previous failure of �2 ICSI cycles
The IMSI outcomes were
matched with ICSI outcomes
from similar couples
ICSI: 9.5
IMSI: 27.9c
ICSI: 30.0
IMSI: 66.0c
ICSI: 33.0
IMSI: 9.0c
2,1,3
[4] Comparative
study
80 80 IF Female age �37 years, >3
retrieved ova, male infertility,
previous failure of �2 ICSI cycles
The IMSI outcomes were
matched with ICSI outcomes
from similar couples
ICSI: 9.4
IMSI: 31.3c
ICSI: 25.0
IMSI: 60.0c
ICSI: 14.0
IMSI: 40.0c
2,1,3
[22] Randomized
study
219 227 MF Female age �35 years, severe
oligoasthenoteratozoo spermia
Couples were randomized to ICSI
and IMSI groups
ICSI: 11.3
IMSI: 17.3c
ICSI: 26.5
IMSI: 39.2c
ICSI: 24.1
IMSI: 16.9a
X
[8] Cohort study 30 30 IF Female age <38 years, previous
failure of �2 ICSI cycles
The IMSI outcomes were
matched with ICSI outcomes
from similar couples
ICSI: 29.7
IMSI: 44.8c
ICSI: 50.0
IMSI: 63.0a
ICSI: 26.6
IMSI: 15.7a
2,1,2
[12] Randomized
study
37 20 MF Poor semen quality and all
arrested embryos following a
prolonged 5-day culture in
previous ICSI cycles
Couples were randomized into
ICSI and IMSI groups
ICSI: 6.8
IMSI: 17.1a
ICSI: 8.1
IMSI: 25.0a
X X
[14] Comparative
study
55 63 IF Female age �39 years, �4
retrieved ova in previous cycles,
previous failure of �2 ICSI cycles
with good quality embryos
Couples were divided into ICSI
and IMSI groups and the
outcomes were compared
ICSI: 9.8
IMSI: 13.6a
ICSI: 19.0
IMSI: 26.0a
ICSI: 31.6
IMSI: 15.4a
3,1,2
Comparative
study
45 37 IF and a
subpopulation
with MF
Female age �39 years, �4
retrieved ova in previous cycles,
patients with male factor with
�2 ICSI attempts
Couples were divided into ICSI
and IMSI groups and the
outcomes were compared
ICSI: 11.2
IMSI: 11.8a
ICSI: 24.4
IMSI: 32.4a
ICSI: 36.4
IMSI: 16.7a
References Design ICSI
cycles
IMSI
cycles
Indication Inclusion criteria Methods Implantation
rate (%)
Pregnancy
rate (%)
Miscarriage
rate (%)
Newcastle–
Ottawa
scale S, C, O
[15] Randomized
study
250 250 MF Isolated male factor infertility,
�6 oocytes available on retrieval
Couples were randomized into
ICSI and IMSI groups
ICSI: 25.4
IMSI: 23.8a
ICSI: 36.8
IMSI: 37.2a
ICSI: 17.9
IMSI: 18.4a
X
[16] Randomized
study
125 125 MF Sperm concentration between
1�106/ml and 20�106/ml
Patients were randomized to ICSI
or IMSI techniques and outcomes
were compared
ICSI: 14.8
IMSI: 24.2c
ICSI: 40.0
IMSI: 65.6c
X X
[11] Randomized
study
70 52 MF Isolated teratozoospermia, �6
mature oocytes available on
retrieval
Patients were randomized to ICSI
or IMSI techniques and outcomes
were compared
ICSI: 29.0
IMSI:16.5c
ICSI: 24.0
IMSI: 48.0c
ICSI: 11.8
IMSI: 20.0a
X
[6] Randomized
study
139 125 MF Female age <38 years, at least 2
and no more than 20 mature
oocytes. Cycles with fresh
ejaculated spermatozoa with
concentration �0.1 million/ml
were included
The oocytes were split into ICSI
(n = 1548) and IMSI groups
(n = 1557) and the fertilization
and percentage of high-quality
embryos were compared
between the groups
ICSI: 32.2
IMSI: 30.3a
ICSI: 36.7
IMSI: 34.4a
ICSI: 2.0
IMSI: 7.0a
X
A.S.
Setti et
al.
/ E
uro
pea
n Jo
urn
al
of
Ob
stetrics &
Gy
neco
log
y a
nd
Rep
rod
uctiv
e B
iolo
gy
18
3 (2
01
4)
96
–1
03
9
9

Table 1 (Continued )
References Design ICSI
cycles
IMSI
cycles
Indication Inclusion criteria Methods Implantation
rate (%)
Pregnancy
rate (%)
Miscarriage
rate (%)
Newcastle–
Ottawa
scale S, C, O
[7] Prospective
non-randomized
study
130 90 IF Couples with mild male factor
who had at least two
implantation failures after
transfers of good-quality
embryos
Couples were divided into ICSI
and IMSI groups and the
outcomes were compared
ICSI: 28.8
IMSI: 34.4a
ICSI: 26.0
IMSI: 24.0a
X 4,1,3
126 132 MF Patients with severe
teratozoospermia at their first or
second attempt
Couples were divided into ICSI
and IMSI groups and the
outcomes were compared
ICSI: 20.1
IMSI: 30.7c
ICSI: 26.0
IMSI: 46.0c
X
References Design ICSI
cycles
IMSI
cycles
Indication Inclusion criteria Methods Implantation
rate (%)
Pregnancy
rate (%)
Miscarriage
rate (%)
Newcastle–
Ottawa
scale S, C, O
[10] Cohort study 322 127 IF Failed fertilization or less than
20% fertilization rate in a
previous IVF treatment, total
motile count <1.5 million after
sperm wash and preparation or
normal morphology of <2%
and>90% head defects (WHO
2010 criteria) or <5% and >90%
head defects
Couples were divided into ICSI
and IMSI groups and the
outcomes were compared
X ICSI: 38.0
IMSI: 56.0c
X 4,1,3
1033 269 MF Failed fertilization or less than
20% fertilization rate in a
previous IVF treatment, total
motile count <1.5 million after
sperm wash and preparation or
normal morphology of <2%
and>90% head defects or <5%
and >90% head defects
Couples were divided into ICSI
and IMSI groups and the
outcomes were compared
X ICSI: 46.0
IMSI: 47.0a
X
Note: IF—implantation failure; MF—male factor.a Not significantly different from ICSI.
bNot applicable.c Significantly different from ICSI.
X—not evaluated; S—selection; C—comparability; O—outcome.
A.S.
Setti et
al.
/ E
uro
pea
n Jo
urn
al
of
Ob
stetrics &
Gy
neco
log
y a
nd
Rep
rod
uctiv
e B
iolo
gy
18
3 (2
01
4)
96
–1
03
10
0

paternal effect reflects DNA contents and can impair embryodevelopment from day 3 to day 5. Several DNA abnormalities havebeen associated with the occurrence of sperm nuclear vacuoles.Consequently, it may be suggested that the improvements inclinical outcomes after IMSI compared with ICSI is explained by anoptimal selection of spermatozoa free of vacuoles having the bestchances to produce a viable blastocyst with higher implantationpotential. In fact, Delaroche et al. [35] recently observed that thenumber of extended embryo culture cycles and the mean numberof blastocysts obtained were higher in IMSI cycles than in ICSIcycles. In a recent study investigating the effects of sperm vacuolesin early and late outcomes, Greco et al. [36] observed thatstatistically significant differences were detected in the ‘‘late’’outcomes, such as pregnancy, implantation, and live birth rates.The use of IMSI has also been associated with decreased likelihoodof malformations in offspring [37,38].
The first meta-analysis on ICSI � IMSI outcomes was publishedin 2010, and concluded that IMSI not only significantly improvesthe percentage of top-quality embryos, implantation and preg-nancy rates, but also significantly reduces miscarriage rates ascompared with ICSI [19]. However, only 3 studies (one randomizedand two nonrandomized studies) that fitted the predetermined
criteria were available at the time. More recently, a new meta-analysis showed that the evidence that IMSI improves clinicalpregnancy is of very low quality [20]. Moreover, no evidence ofeffect on live birth or miscarriage was observed. The authorssuggested that further trials are necessary to improve the evidencequality before recommending IMSI in clinical practice. One couldargue why this previous meta-analysis and ours have suchdifferent results and recommendations, given that only random-ized clinical trials were included in Teixeira’s study and thereforeour grounds are less solid. The meta-analysis of Teixeira et al. didnot take into account the indications for ICSI; therefore, theirresults cannot be generalized for all the couples undergoing ICSIwhich might explain the discrepancies in the findings andconclusions.
A weakness of this meta-analysis is related to the lack ofconsensus among the included studies regarding the number ofprevious ICSI attempts and the definition of male factor, whichcould have introduced a bias. In addition, prior failures in ICSIcycles constituted an inclusion criterion in several studiesemploying IMSI. Additionally, the implantation rate may beunderestimated because it was not calculate per patient but pertransferred embryos.
Fig. 2. Meta-analysis. Results are expressed as odds ratios (OR) with 95% of confidence intervals (CI). Fixed and random models assume homogenous and heterogeneous
studies, respectively.
A.S. Setti et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 183 (2014) 96–103 101
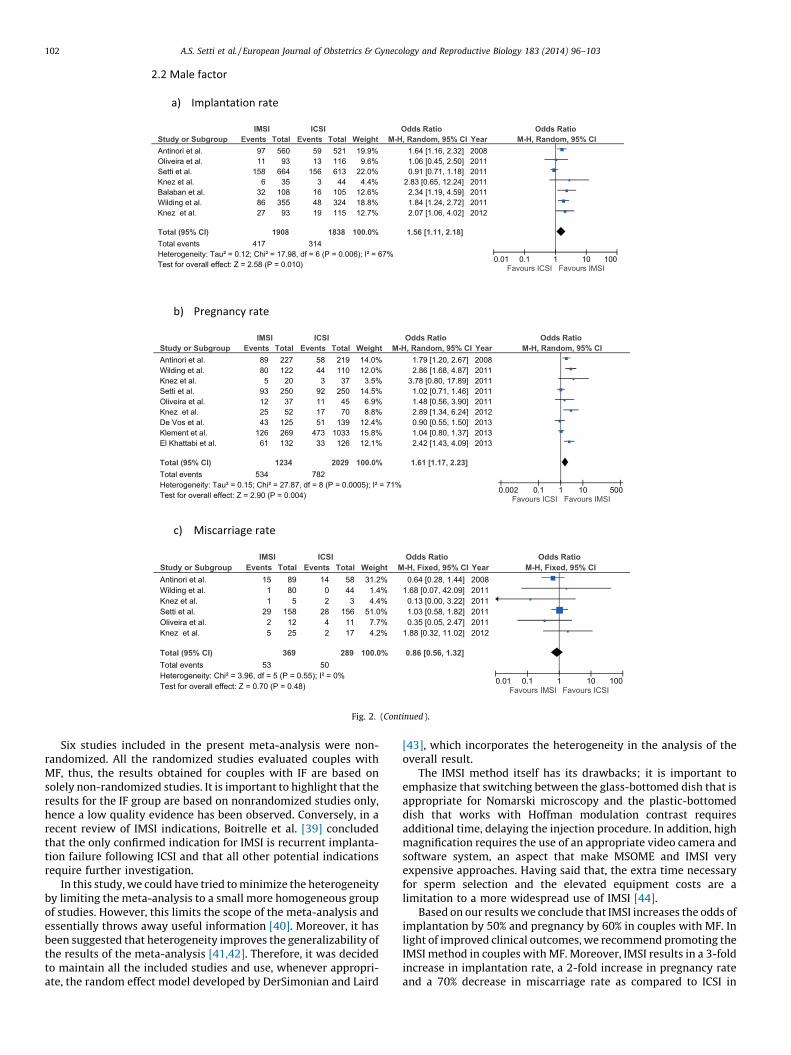
Six studies included in the present meta-analysis were non-randomized. All the randomized studies evaluated couples withMF, thus, the results obtained for couples with IF are based onsolely non-randomized studies. It is important to highlight that theresults for the IF group are based on nonrandomized studies only,hence a low quality evidence has been observed. Conversely, in arecent review of IMSI indications, Boitrelle et al. [39] concludedthat the only confirmed indication for IMSI is recurrent implanta-tion failure following ICSI and that all other potential indicationsrequire further investigation.
In this study, we could have tried to minimize the heterogeneityby limiting the meta-analysis to a small more homogeneous groupof studies. However, this limits the scope of the meta-analysis andessentially throws away useful information [40]. Moreover, it hasbeen suggested that heterogeneity improves the generalizability ofthe results of the meta-analysis [41,42]. Therefore, it was decidedto maintain all the included studies and use, whenever appropri-ate, the random effect model developed by DerSimonian and Laird
[43], which incorporates the heterogeneity in the analysis of theoverall result.
The IMSI method itself has its drawbacks; it is important toemphasize that switching between the glass-bottomed dish that isappropriate for Nomarski microscopy and the plastic-bottomeddish that works with Hoffman modulation contrast requiresadditional time, delaying the injection procedure. In addition, highmagnification requires the use of an appropriate video camera andsoftware system, an aspect that make MSOME and IMSI veryexpensive approaches. Having said that, the extra time necessaryfor sperm selection and the elevated equipment costs are alimitation to a more widespread use of IMSI [44].
Based on our results we conclude that IMSI increases the odds ofimplantation by 50% and pregnancy by 60% in couples with MF. Inlight of improved clinical outcomes, we recommend promoting theIMSI method in couples with MF. Moreover, IMSI results in a 3-foldincrease in implantation rate, a 2-fold increase in pregnancy rateand a 70% decrease in miscarriage rate as compared to ICSI in
Fig. 2. (Continued ).
A.S. Setti et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 183 (2014) 96–103102
couples with IF, however, as no randomized evidence exists,randomized studies are needed to confirm the IMSI benefits incouples with IF.
Condensation
IMSI increases the odds of implantation by 50% and pregnancyby 60% in couples with MF, and results in a 3-fold increase inimplantation rate, a 2-fold increase in pregnancy rate and a 70%decrease in miscarriage rate as compared to ICSI in couples with IF.
References
[1] Bartoov B, Berkovitz A, Eltes F. Selection of spermatozoa with normal nuclei toimprove the pregnancy rate with intracytoplasmic sperm injection. N Engl JMed 2001;345:1067–8.
[2] Bartoov B, Berkovitz A, Eltes F, et al. Pregnancy rates are higher with intra-cytoplasmic morphologically selected sperm injection than with conventionalintracytoplasmic injection. Fertil Steril 2003;80:1413–9.
[3] Bartoov B, Berkovitz A, Eltes F, Kogosowski A, Menezo Y, Barak Y. Real-time finemorphology of motile human sperm cells is associated with IVF-ICSI outcome.J Androl 2002;23:1–8.
[4] Berkovitz A, Eltes F, Ellenbogen A, Peer S, Feldberg D, Bartoov B. Does thepresence of nuclear vacuoles in human sperm selected for ICSI affect pregnan-cy outcome? Hum Reprod 2006;21:1787–90.
[5] Berkovitz A, Eltes F, Lederman H, et al. How to improve IVF-ICSI outcome bysperm selection. Reprod Biomed Online 2006;12:634–8.
[6] De Vos A, Van de Velde H, Bocken G, et al. Does intracytoplasmic morphologi-cally selected sperm injection improve embryo development? A randomizedsibling-oocyte study. Hum Reprod 2013;28:617–26.
[7] El Khattabi L, Dupont C, Sermondade N, et al. Is intracytoplasmic morphologicallyselected sperm injection effective in patients with infertility related to terato-zoospermia or repeated implantation failure? Fertil Steril 2013;100:62–8.
[8] Gonzalez-Ortega C, Cancino-Villarreal P, Perez-Torres A, et al. Intracytoplasmicmorphologically selected sperm injection (IMSI) vs intracytoplasmic sperminjection (ICSI) in patients with repeated ICSI failure. Ginecol Obstet Mex2010;78:652–9.
[9] Hazout A, Dumont-Hassan M, Junca AM, Cohen Bacrie P, Tesarik J. High-magnification ICSI overcomes paternal effect resistant to conventional ICSI.Reprod Biomed Online 2006;12:19–25.
[10] Klement AH, Koren-Morag N, Itsykson P, Berkovitz A. Intracytoplasmic mor-phologically selected sperm injection versus intracytoplasmic sperm injec-tion: a step toward a clinical algorithm. Fertil Steril 2013;99:1290–3.
[11] Knez K, Tomazevic T, Zorn B, Vrtacnik-Bokal E, Virant-Klun I. Intracytoplasmicmorphologically selected sperm injection improves development and qualityof preimplantation embryos in teratozoospermia patients. Reprod BiomedOnline 2012;25:168–79.
[12] Knez K, Zorn B, Tomazevic T, Vrtacnik-Bokal E, Virant-Klun I. The IMSIprocedure improves poor embryo development in the same infertile coupleswith poor semen quality: a comparative prospective randomized study.Reprod Biol Endocrinol 2011;9:123.
[13] Mauri AL, Petersen CG, Oliveira JB, Massaro FC, Baruffi RL, Franco Jr JG.Comparison of day 2 embryo quality after conventional ICSI versus intracy-toplasmic morphologically selected sperm injection (IMSI) using siblingoocytes. Eur J Obstet Gynecol Reprod Biol 2010;150:42–6.
[14] Oliveira JB, Cavagna M, Petersen CG, et al. Pregnancy outcomes in women withrepeated implantation failures after intracytoplasmic morphologically select-ed sperm injection (IMSI). Reprod Biol Endocrinol 2011;9:99.
[15] Setti AS, Figueira Rde C, Braga DP, Iaconelli Jr A, Borges Jr E. Intracytoplasmicmorphologically selected sperm injection benefits for patients with oli-goasthenozoospermia according to the 2010 World Health Organizationreference values. Fertil Steril 2011;95:2711–4.
[16] Wilding M, Coppola G, di Matteo L, Palagiano A, Fusco E, Dale B. Intracyto-plasmic injection of morphologically selected spermatozoa (IMSI) improvesoutcome after assisted reproduction by deselecting physiologically poorquality spermatozoa. J Assist Reprod Genet 2011;28:253–62.
[17] Berkovitz A, Eltes F, Soffer Y, et al. ART success and in vivo sperm cellselection depend on the ultramorphological status of spermatozoa. Andro-logia 1999;31:1–8.
[18] Berkovitz A, Eltes F, Yaari S, et al. The morphological normalcy of the spermnucleus and pregnancy rate of intracytoplasmic injection with morphologi-cally selected sperm. Hum Reprod 2005;20:185–90.
[19] Souza Setti A, Ferreira RC, Paes de Almeida Ferreira Braga D, de Cassia SavioFigueira R, Iaconelli Jr A, Borges Jr E. Intracytoplasmic sperm injection outcomeversus intracytoplasmic morphologically selected sperm injection outcome: ameta-analysis. Reprod Biomed Online 2010;21:450–5.
[20] Teixeira DM, Barbosa MA, Ferriani RA, et al. Regular (ICSI) versus ultra-highmagnification (IMSI) sperm selection for assisted reproduction. CochraneDatabase Syst Rev 2013;7:CD010167.
[21] Wells G. The Newcastle Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analysis. In: Proceedings of the third symposiumon systematic reviews beyond the basics: improving quality and impact; 2000.
[22] Antinori M, Licata E, Dani G, et al. Intracytoplasmic morphologically selectedsperm injection: a prospective randomized trial. Reprod Biomed Online2008;16:835–41.
[23] Boitrelle F, Albert M, Theillac C, et al. Cryopreservation of human spermatozoadecreases the number of motile normal spermatozoa, induces nuclear vacuo-lization and chromatin decondensation. J Androl 2012;33:1371–8.
[24] Cassuto NG, Hazout A, Hammoud I, et al. Correlation between DNA defect andsperm-head morphology. Reprod Biomed Online 2012;24:211–8.
[25] de Almeida Ferreira Braga DP, Setti AS, Figueira RC, et al. Sperm organellemorphologic abnormalities: contributing factors and effects on intracytoplas-mic sperm injection cycles outcomes. Urology 2011;78:786–91.
[26] Franco Jr JG, Mauri AL, Petersen CG, et al. Large nuclear vacuoles are indicativeof abnormal chromatin packaging in human spermatozoa. Int J Androl2012;35:46–51.
[27] Perdrix A, Saidi R, Menard JF, et al. Relationship between conventional spermparameters and motile sperm organelle morphology examination (MSOME).Int J Androl 2012;35:491–8.
[28] Setti AS, Figueira RC, Braga DP, Iaconelli Jr A, Borges Jr E. Gender incidence ofintracytoplasmic morphologically selected sperm injection-derived embryos:a prospective randomized study. Reprod Biomed Online 2012;24:420–3.
[29] Silva LF, Oliveira JB, Petersen CG, et al. The effects of male age on spermanalysis by motile sperm organelle morphology examination (MSOME).Reprod Biol Endocrinol 2012;10:19.
[30] Vanderzwalmen P, Hiemer A, Rubner P, et al. Blastocyst development aftersperm selection at high magnification is associated with size and number ofnuclear vacuoles. Reprod Biomed Online 2008;17:617–27.
[31] Marci R, Murisier F, Lo Monte G, et al. Clinical outcome after IMSI procedure inan unselected infertile population: a pilot study. Reprod Health 2013;10:16.
[32] Setti AS, Braga DP, Figueira RC, Iaconelli Jr A, Borges Jr E. The predictive valueof high-magnification sperm morphology examination on ICSI outcomes in thepresence of oocyte dysmorphisms. J Assist Reprod Genet 2011;29:1241–7.
[33] Balaban B, Yakin K, Alatas C, Oktem O, Isiklar A, Urman B. Clinical outcome ofintracytoplasmic injection of spermatozoa morphologically selected underhigh magnification: a prospective randomized study. Reprod Biomed Online2011;22:472–6.
[34] Barroso G, Valdespin C, Vega E, et al. Developmental sperm contributions:fertilization and beyond. Fertil Steril 2009;92:835–48.
[35] Delaroche L, Yazbeck C, Gout C, Kahn V, Oger P, Rougier N. Intracytoplasmicmorphologically selected sperm injection (IMSI) after repeated IVF or ICSIfailures: a prospective comparative study. Eur J Obstet Gynecol Reprod Biol2013;167:76–80.
[36] Greco E, Scarselli F, Fabozzi G, et al. Sperm vacuoles negatively affect outcomesin intracytoplasmic morphologically selected sperm injection in terms ofpregnancy, implantation, and live-birth rates. Fertil Steril 2013;100:379–85.
[37] Berkovitz A, Eltes F, Paul M, Adrian E, Bartoov B. The chance of having a healthynormal child following intracytoplasmic morphologically-selected sperm in-jection (IMSI) treatment is higher compared to conventional IVF-ICSI treat-ment. Fertil Steril 2007;88:S20.
[38] Cassuto NG, Hazout A, Bouret D, et al. Low birth defects by deselectingabnormal spermatozoa before ICSI. Reprod Biomed Online 2014;28:47–53.
[39] Boitrelle F, Guthauser B, Alter L, et al. High-magnification selection of sper-matozoa prior to oocyte injection: confirmed and potential indications.Reprod Biomed Online 2014;28:6–13.
[40] Berman NG, Parker RA. Meta-analysis: neither quick nor easy. BMC Med ResMethodol 2002;2:10.
[41] Biggerstaff BJ, Tweedie RL. Incorporating variability in estimates of het-erogeneity in the random effects model in meta-analysis. Stat Med1997;16:753–68.
[42] Dickersin K, Min YI, Meinert CL. Factors influencing publication of researchresults. Follow-up of applications submitted to two institutional reviewboards. JAMA 1992;267:374–8.
[43] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials1986;7:177–88.
[44] Setti AS, Paes de Almeida Ferreira Braga D, Iaconelli Jr A, Aoki T, Borges Jr E.Twelve years of MSOME and IMSI: a review. Reprod Biomed Online2013;27:338–52.
A.S. Setti et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 183 (2014) 96–103 103

14
5. CONSIDERAÇÕES FINAIS
15
O artigo publicado trata-se da primeira meta-análise que compara os
resultados de ICSI e IMSI em casais com fator masculino de infertilidade e falha
prévia de ICSI.
Os resultados da presente meta-análise para as taxas de implantação e
gestação foram a favor da IMSI em casais com fator masculino de infertilidade.
Ainda, os resultados da meta-análise para as taxas de implantação, gestação e
aborto foram a favor da IMSI em casais com falha prévia de ICSI.
É importante ressaltar que os resultados observados para casais com falha
prévia de ICSI foram baseados em seis estudos não randomizados, portanto, a
evidência deve ser considerada de baixa qualidade. Por outro lado, os resultados
observados para casais com fator masculino de infertilidade foram baseados em
sete estudos randomizados, garantindo assim uma evidência de alta qualidade.
A IMSI quando comparada à ICSI resulta em taxa de implantação três vezes
maior, taxa de gestação duas vezes maior e taxa de aborto 70% menor em casais
com falha prévia de ICSI. Entretanto, devido à baixa qualidade da evidência, os
benefícios da técnica de IMSI nesses casais ainda precisam ser confirmados em
ensaios randomizados.
A IMSI aumenta a chance de implantação e gestação em 50% e 60%,
respectivamente, em casais com fator masculino de infertilidade e, esta evidência de
alta qualidade sugere que a técnica pode ser introduzida na rotina com segurança,
trazendo benefícios para esses casais.

16
6. CONCLUSÕES

17
Conclui-se que a IMSI quando comparada com a ICSI:
• Melhora as taxas de implantação, gestação e aborto em casais com
falha prévia de ICSI;
• Melhora as taxas de implantação e gestação, porém não melhora as
taxas de aborto em casais com fator masculino de infertilidade.

18
7. REFERÊNCIAS BIBLOGRÁFICAS
19
Antinori M, Licata E, Dani G, Cerusico F, Versaci C, d'Angelo D, Antinori S.
Intracytoplasmic morphologically selected sperm injection: a prospective randomized
trial. Reprod Biomed Online. 2008;16:835-41.
Balaban B, Yakin K, Alatas C, Oktem O, Isiklar A, Urman B. Clinical outcome of
intracytoplasmic injection of spermatozoa morphologically selected under high
magnification: a prospective randomized study. Reprod Biomed Online. 2011;22:472-
76.
Bartoov B, Berkovitz A, Eltes F. Selection of spermatozoa with normal nuclei to
improve the pregnancy rate with intracytoplasmic sperm injection. N Engl J Med.
2001;345:1067-8.
Bartoov B, Berkovitz A, Eltes F, Kogosovsky A, Yagoda A, Lederman H, Artzi S,
Gross M, Barak Y. Pregnancy rates are higher with intracytoplasmic morphologically
selected sperm injection than with conventional intracytoplasmic injection. Fertil
Steril. 2003;80:1413-9.
Bartoov B, Berkovitz A, Eltes F, Kogosowski A, Menezo Y, Barak Y. Real-time fine
morphology of motile human sperm cells is associated with IVF-ICSI outcome. J
Androl. 2002;23:1-8.
Berkovitz A, Eltes F, Lederman H, Peer S, Ellenbogen A, Feldberg B, Bartoov B.
How to improve IVF-ICSI outcome by sperm selection. Reprod Biomed Online.
2006;12:634-8.
Berkovitz A, Eltes F, Soffer Y, Zabludovsky N, Beyth Y, Farhi J, Levran D, Bartoov B.
ART success and in vivo sperm cell selection depend on the ultramorphological
status of spermatozoa. Andrologia. 1999;31:1-8.
Borini A, Tarozzi N, Bizzaro D, Bonu MA, Fava L, Flamigni C, Coticchio G. Sperm
DNA fragmentation: paternal effect on early post-implantation embryo development
in ART. Hum Reprod. 2006;21:2876-81.
20
De Vos A, Van de Velde H, Bocken G, Eylenbosch G, Franceus N, Meersdom G,
Tistaert S, Vankelecom A, Tournaye H, Verheyen G. Does intracytoplasmic
morphologically selected sperm injection improve embryo development? A
randomized sibling-oocyte study. Hum Reprod. 2013;28:617-26.
El Khattabi L, Dupont C, Sermondade N, Hugues JN, Poncelet C, Porcher R, Cedrin-
Durnerin I, Levy R, Sifer C. Is intracytoplasmic morphologically selected sperm
injection effective in patients with infertility related to teratozoospermia or repeated
implantation failure? Fertil Steril. 2013;100:62-8.
Figueira Rde C, Braga DP, Setti AS, Iaconelli A, Jr., Borges E, Jr. Morphological
nuclear integrity of sperm cells is associated with preimplantation genetic aneuploidy
screening cycle outcomes. Fertil Steril. 2011;95:990-3.
Franco JG, Jr., Baruffi RL, Mauri AL, Petersen CG, Oliveira JB, Vagnini L.
Significance of large nuclear vacuoles in human spermatozoa: implications for ICSI.
Reprod Biomed Online. 2008;17:42-5.
Garolla A, Fortini D, Menegazzo M, De Toni L, Nicoletti V, Moretti A, Selice R, Engl
B, Foresta C. High-power microscopy for selecting spermatozoa for ICSI by
physiological status. Reprod Biomed Online. 2008;17:610-6.
Gonzalez-Ortega C, Cancino-Villarreal P, Perez-Torres A, Vargas-Maciel MA,
Martinez-Garza SG, Perez-Pena E, Gutierrez-Gutiedrrez AM. Intracytoplasmic
morphologically selected sperm injection (IMSI) vs intracytoplasmic sperm injection
(ICSI) in patients with repeated ICSI failure. Ginecol Obstet Mex. 2010;78:652-9.
Hazout A, Dumont-Hassan M, Junca AM, Cohen Bacrie P, Tesarik J. High-
magnification ICSI overcomes paternal effect resistant to conventional ICSI. Reprod
Biomed Online. 2006;12:19-25.
21
Klement AH, Koren-Morag N, Itsykson P, Berkovitz A. Intracytoplasmic
morphologically selected sperm injection versus intracytoplasmic sperm injection: a
step toward a clinical algorithm. Fertil Steril. 2013;99:1290-3.
Knez K, Tomazevic T, Zorn B, Vrtacnik-Bokal E, Virant-Klun I. Intracytoplasmic
morphologically selected sperm injection improves development and quality of
preimplantation embryos in teratozoospermia patients. Reprod Biomed Online.
2012;25:168-79.
Knez K, Zorn B, Tomazevic T, Vrtacnik-Bokal E, Virant-Klun I. The IMSI procedure
improves poor embryo development in the same infertile couples with poor semen
quality: a comparative prospective randomized study. Reprod Biol Endocrinol.
2011;9:123.
Kruger TF, Acosta AA, Simmons KF, Swanson RJ, Matta JF, Oehninger S. Predictive
value of abnormal sperm morphology in in vitro fertilization. Fertil Steril. 1988;49:112-
7.
Kupker W, al-Hasani S, Schulze W, Kuhnel W, Schill T, Felberbaum R, Diedrich K.
Morphology in intracytoplasmic sperm injection: preliminary results. J Assist Reprod
Genet. 1995;12:620-6.
Liu DY, Baker HW. Sperm nuclear chromatin normality: relationship with sperm
morphology, sperm-zona pellucida binding, and fertilization rates in vitro. Fertil Steril.
1992;58:1178-84.
Lundin K, Soderlund B, Hamberger L. The relationship between sperm morphology
and rates of fertilization, pregnancy and spontaneous abortion in an in-vitro
fertilization/intracytoplasmic sperm injection programme. Hum Reprod.
1997;12:2676-81.
22
Mansour RT, Aboulghar MA, Serour GI, Amin YM, Ramzi AM. The effect of sperm
parameters on the outcome of intracytoplasmic sperm injection. Fertil Steril.
1995;64:982-6.
Mashiach R, Fisch B, Eltes F, Tadir Y, Ovadia J, Bartoov B. The relationship between
sperm ultrastructural features and fertilizing capacity in vitro. Fertil Steril.
1992;57:1052-7.
Nagy ZP, Liu J, Joris H, Verheyen G, Tournaye H, Camus M, Derde MC, Devroey P,
Van Steirteghem AC. The result of intracytoplasmic sperm injection is not related to
any of the three basic sperm parameters. Hum Reprod. 1995;10:1123-9.
Oliveira JB, Cavagna M, Petersen CG, Mauri AL, Massaro FC, Silva LF, Baruffi RL,
Franco JG, Jr. Pregnancy outcomes in women with repeated implantation failures
after intracytoplasmic morphologically selected sperm injection (IMSI). Reprod Biol
Endocrinol. 2011;9:99.
Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after
intracytoplasmic injection of single spermatozoon into an oocyte. Lancet.
1992;340:17-8.
Setti AS, Figueira Rde C, Braga DP, Iaconelli A, Jr., Borges E, Jr. Intracytoplasmic
morphologically selected sperm injection benefits for patients with
oligoasthenozoospermia according to the 2010 World Health Organization reference
values. Fertil Steril. 2011;95:2711-4.
Souza Setti A, Ferreira RC, Paes de Almeida Ferreira Braga D, de Cassia Savio
Figueira R, Iaconelli A, Jr., Borges E, Jr. Intracytoplasmic sperm injection outcome
versus intracytoplasmic morphologically selected sperm injection outcome: a meta-
analysis. Reprod Biomed Online. 2010;21:450-5.
23
Sukcharoen N, Sithipravej T, Promviengchai S, Chinpilas V, Boonkasemsanti W.
Sperm morphology evaluated by computer (IVOS) cannot predict the fertilization rate
in vitro after intracytoplasmic sperm injection. Fertil Steril. 1998;69:564-8.
Svalander P, Jakobsson AH, Forsberg AS, Bengtsson AC, Wikland M. The outcome
of intracytoplasmic sperm injection is unrelated to 'strict criteria' sperm morphology.
Hum Reprod. 1996;11:1019-22.
Teixeira DM, Barbosa MA, Ferriani RA, Navarro PA, Raine-Fenning N, Nastri CO,
Martins WP. Regular (ICSI) versus ultra-high magnification (IMSI) sperm selection for
assisted reproduction. Cochrane Database Syst Rev. 2013;7:CD010167.
Tesarik J. Paternal effects on cell division in the human preimplantation embryo.
Reprod Biomed Online. 2005;10:370-5.
Tesarik J, Greco E, Mendoza C. Late, but not early, paternal effect on human embryo
development is related to sperm DNA fragmentation. Hum Reprod. 2004;19:611-5.
Tesarik J, Mendoza C, Greco E. Paternal effects acting during the first cell cycle of
human preimplantation development after ICSI. Hum Reprod. 2002;17:184-9.
Vanderzwalmen P, Fallet C. [IMSI: indications, results and reflexions]. J Gynecol
Obstet Biol Reprod (Paris). 2008;39:22-5.
Wilding M, Coppola G, di Matteo L, Palagiano A, Fusco E, Dale B. Intracytoplasmic
injection of morphologically selected spermatozoa (IMSI) improves outcome after
assisted reproduction by deselecting physiologically poor quality spermatozoa. J
Assist Reprod Genet. 2011;28:253-62.
Zini A, Bielecki R, Phang D, Zenzes MT. Correlations between two markers of sperm
DNA integrity, DNA denaturation and DNA fragmentation, in fertile and infertile men.
Fertil Steril. 2001;75:674-7.