CLEBER VELOSO DE CARVALHO - s3.amazonaws.com · angiotensina (eca), atividade fÍsica e...
63
Londrina 2013 CENTRO DE PESQUISA EM CIÊNCIAS DA SAÚDE MESTRADO EM CIÊNCIAS DA REABILITAÇÃO CLEBER VELOSO DE CARVALHO ESTUDO DE ASSOCIAÇÃO DO TIPO CASO CONTROLE ENTRE O POLIMORFISMO DE INSERÇÃO/DELEÇÃO (RS4646994) NO GENE DA ENZIMA CONVERSORA DE ANGIOTENSINA (ECA), ATIVIDADE FÍSICA E HIPERTENSÃO ESSENCIAL EM IDOSOS
Transcript of CLEBER VELOSO DE CARVALHO - s3.amazonaws.com · angiotensina (eca), atividade fÍsica e...
Londrina 2013
CENTRO DE PESQUISA EM CIÊNCIAS DA SAÚDE MESTRADO EM CIÊNCIAS DA REABILITAÇÃO
CLEBER VELOSO DE CARVALHO
ESTUDO DE ASSOCIAÇÃO DO TIPO CASO CONTROLE ENTRE O POLIMORFISMO DE INSERÇÃO/DELEÇÃO
(RS4646994) NO GENE DA ENZIMA CONVERSORA DE ANGIOTENSINA (ECA), ATIVIDADE FÍSICA E HIPERTENSÃO
ESSENCIAL EM IDOSOS
Londrina 2013
CLEBER VELOSO DE CARVALHO
ESTUDO DE ASSOCIAÇÃO DO TIPO CASO CONTROLE ENTRE O POLIMORFISMO DE INSERÇÃO/DELEÇÃO
(RS4646994) NO GENE DA ENZIMA CONVERSORA DE ANGIOTENSINA (ECA), ATIVIDADE FISÍCA E HIPERTENSÃO
ESSENCIAL EM IDOSOS
Dissertação apresentada ao Programa de Pós-Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina - UEL e Universidade Norte do Paraná - UNOPAR), como requisito parcial à obtenção do título de Mestre em Ciências da Reabilitação.
Orientadora: Profª. Drª. Regina Célia Poli- Frederico
AUTORIZO A REPRODUÇÃO TOTAL OU PARCIAL DESTE TRABALHO, POR QUALQUER MEIO CONVENCIONAL OU ELETRÔNICO, PARA FINS DE ESTUDO E PESQUISA, DESDE QUE CITADA A FONTE.
Dados Internacionais de catalogação-na-publicação Universidade Norte do Paraná
Biblioteca Central
Setor de Tratamento da Informação
Carvalho, Cleber Veloso de.
C322e Estudo de associação do tipo caso controle entre o polimorfismo de inserção
/deleção (RS 4646994) no gene da enzima conversora de angiotensina (ECA),
atividade física e hipertensão essencial em idosos / Cleber Veloso de Carvalho.
Londrina: [s.n], 2013.
xi; 60p.
Dissertação (Mestrado). Ciências da Reabilitação. Universidade Norte do Paraná e
Universidade Estadual de Londrina.
Orientadora: Profª Drª. Regina Célia Poli-Frederico.
1- Ciências da reabilitação - dissertação de mestrado – UNOPAR/UEL 2- Hipertensão 3-
RS4646994 4- Polimorfismo genético 5- Enzima conversora de angiotensina 6-
Idosos 7- Capacidade de exercício 8- Capacidade funcional I- Poli-Frederico,
Regina Célia, orient. II- Universidade Norte do Paraná. III- Universidade
Estadual de Londrina.
CDU 615.8:612

CLEBER VELOSO DE CARVALHO
ESTUDO DE ASSOCIAÇÃO DO TIPO CASO CONTROLE ENTRE O POLIMORFISMO DE INSERÇÃO/DELEÇÃO
(RS4646994) NO GENE DA ENZIMA CONVERSORA DE ANGIOTENSINA (ECA), ATIVIDADE FÍSICA E HIPERTENSÃO
ESSENCIAL EM IDOSOS
Dissertação apresentada ao Programa de Pós-Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina [UEL] e Universidade Norte do Paraná [UNOPAR]), como requisito parcial à obtenção do título de Mestre em Ciências da Reabilitação.
BANCA EXAMINADORA
Drª. Regina Célia Poli-
Frederico
Universidade Norte do
Paraná
Drª. Vanessa Suziane
Probst Universidade Norte
do Paraná
Drª. Roberta Losi
Guembarovski Universidade
Estadual de Londrina
Londrina, 26 de Fevereiro de 2013.

AGRADECIMENTOS
Primeiramente agradeço a Deus, pela minha vida e por me ajudar sempre
nessa jornada aqui na terra.
Agradeço, especialmente, a minha orientadora Prof. Dra. Regina Célia Poli-
Frederico pela oportunidade, e por ser essa pessoa maravilhosa, estando sempre
disposta a ajudar e ensinar. Meus sinceros agradecimentos, admiração e respeito.
Sou muito grato a minha namorada, Maristela, pelo seu amor e apoio em
todos os momentos. Obrigado por compreender os momentos de ausência, aos
longos períodos de estudos, as horas dedicadas ao computador nos ajustes da
dissertação.
Sou grato aos colegas de laboratório, Lucio Carvalho, Senhorita Ruzzon,
Cintia Martignago e Louhana Lima, pelos bons momentos que passamos juntos
entre as aulas e o laboratório de Biologia molecular. Em especial agradeço a Bruna
Garbelini pelas valiosas contribuições nas extrações de DNA.
Agradeço aos meus pais Maria Helena Veloso de Carvalho e Severino
Clemente de Carvalho (In memoriam) por sempre acreditarem em mim.
Aos meus irmãos que estavam presentes mesmo não sabendo direito o que
eu estava fazendo.
Sou grato a todos os professores deste programa de Mestrado, que lutam e
estão lutando para a qualidade do programa.
Aos professores da banca, Drª. Vanessa Suziane Probst e Drª. Roberta Losi
Guembarovski, pela valiosa contribuição para a realização deste trabalho.

“É somente nas misteriosas equações do amor que qualquer lógica ou razão pode ser encontrada”
John Nash
CARVALHO, Cleber Veloso. Estudo de associação do tipo caso controle entre o polimorfismo de inserção/deleção (rs4646994) no gene da enzima conversora de angiotensina (ECA), atividade física e hipertensão essencial em idosos. 2013. 58 fls. Dissertação (Mestrado em Ciências da Reabilitação) - Universidade Norte do Paraná, Londrina, 2013.
RESUMO
Introdução: A Hipertensão essencial (HE) é uma doença multifatorial
desencadeada por fatores genéticos e ambientais. A enzima conversora de
angiotensina (ECA) catalisa a conversão da angiotensina I em angiotensina II
(vasoconstritor), assim como realiza a inativação da bradicinina (vasodilatador).
Ambas, a angiotensina II e a bradicinina têm efeitos agudos e crônicos no sistema
cardiovascular. O gene da ECA é caracterizado pela inserção (I) ou deleção (D) de
uma sequência de repetição Alu no intron 16, alterando os níveis plasmáticos da
enzima e consequentemente tem um papel fundamental na homeostasia da
pressão arterial. O polimorfismo I/D no gene da ECA tem sido avaliado quanto ao
seu papel na determinação da preferência pela atividade física. Então seria
possível que, dado um determinado genótipo I/D do gene da ECA, um indivíduo
poderia ser mais propenso à atividade física e consequentemente isto levaria a
uma proteção contra a hipertensão. O objetivo do presente estudo foi avaliar se os
idosos com um determinado polimorfismo I/D no gene da ECA apresentam melhor
capacidade de exercício e se os mesmos são menos propensos a HE. Métodos: A
amostra foi composta por 57 idosos normotensos e 57 hipertensos pareados por
sexo e idade. A genotipagem foi realizada pela reação em cadeia da polimerase
(PCR), com análise dos fragmentos em gel de agarose. A capacidade de exercício
foi avaliada por meio do teste de caminhada de 6 minutos (TC6). A hipertensão foi
diagnosticada de acordo com padrões preconizados pela Organização Mundial da
Saúde (WHO/ISH, 1999). O teste Qui-quadrado foi utilizado para investigar a
associação entre hipertensão e as características demográficas, índice de massa
corporal (IMC), TC6 e a frequência do polimorfismo I/D do gene da ECA, assim
como, para avaliar se a frequência genotípica estava no equilíbrio de Hardy-
Weinberg. A influência do polimorfismo genético e da capacidade de exercício
sobre a hipertensão foi avaliada pela análise de razão de chance (OR) e intervalo
de confiança (IC) de 95%, obtida por regressão logística. O nível de significância
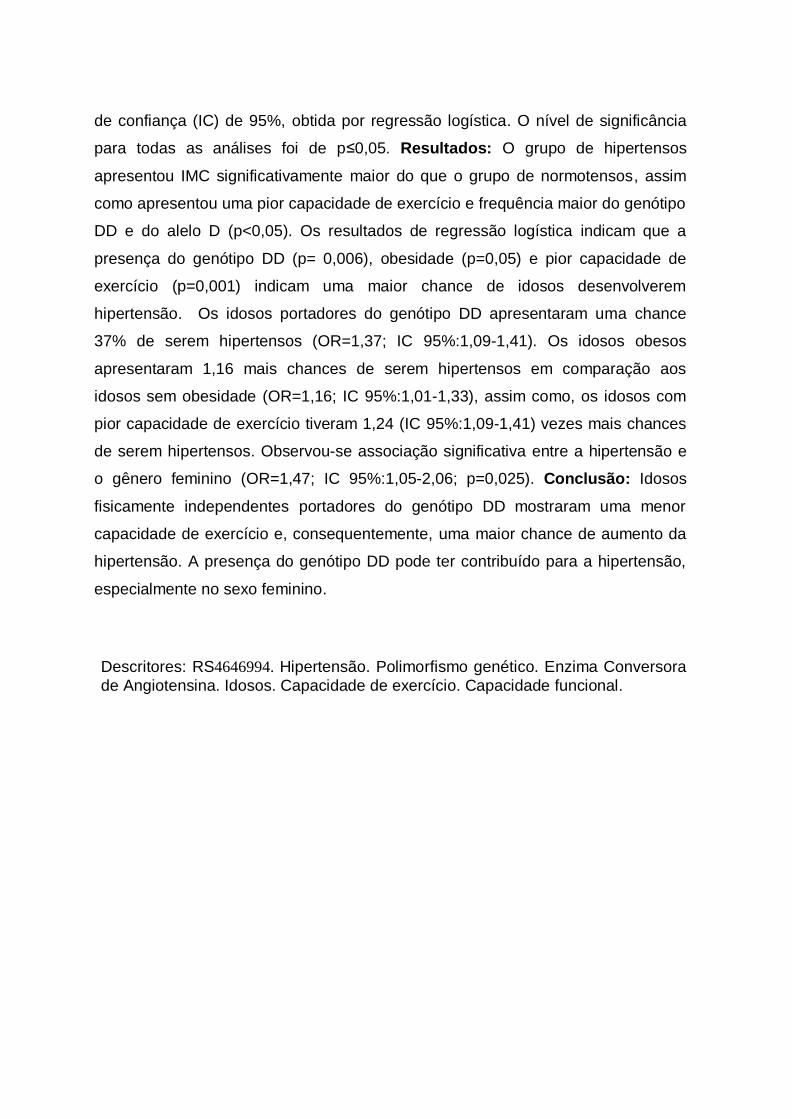
para todas as análises foi de p≤0,05. Resultados: O grupo de hipertensos
apresentou IMC significativamente maior do que o grupo de normotensos, assim
como apresentou uma pior capacidade de exercício e frequência maior do genótipo
DD e do alelo D (p<0,05). Os resultados de regressão logística indicam que a
presença do genótipo DD (p= 0,006), obesidade (p=0,05) e pior capacidade de
exercício (p=0,001) indicam uma maior chance de idosos desenvolverem
hipertensão. Os idosos portadores do genótipo DD apresentaram uma chance
37% de serem hipertensos (OR=1,37; IC 95%:1,09-1,41). Os idosos obesos
apresentaram 1,16 mais chances de serem hipertensos em comparação aos
idosos sem obesidade (OR=1,16; IC 95%:1,01-1,33), assim como, os idosos com
pior capacidade de exercício tiveram 1,24 (IC 95%:1,09-1,41) vezes mais chances
de serem hipertensos. Observou-se associação significativa entre a hipertensão e
o gênero feminino (OR=1,47; IC 95%:1,05-2,06; p=0,025). Conclusão: Idosos
fisicamente independentes portadores do genótipo DD mostraram uma menor
capacidade de exercício e, consequentemente, uma maior chance de aumento da
hipertensão. A presença do genótipo DD pode ter contribuído para a hipertensão,
especialmente no sexo feminino.
Descritores: RS4646994. Hipertensão. Polimorfismo genético. Enzima Conversora
de Angiotensina. Idosos. Capacidade de exercício. Capacidade funcional.
CARVALHO, Cleber Veloso. Estudo de associação do tipo caso controle entre o polimorfismo de inserção/deleção (rs4646994) no gene da enzima conversora de angiotensina (ECA), atividade física e hipertensão essencial em idosos. 2013. 58 fls. Dissertação (Mestrado em Ciências da Reabilitação) - Universidade Norte do Paraná, Londrina, 2013.
ABSTRACT
Background: The Essential hypertension (EH) is a multifactorial disease triggered by
genetic and environmental factors. The angiotensin converting enzyme (ACE)
catalyzes the conversion of angiotensin I to angiotensin II (vasoconstrictor) and
performs the inactivation of bradykinin (vasodilator). Both angiotensin II and bradykinin
have acute and chronic effects on the cardiovascular system. The ACE gene is
characterized by the insertion (I) or deletion (D) of an Alu repeat sequence in intron 16
and, this change in plasma levels of the enzyme and thus have a fundamental role in
the homeostasis of blood pressure. The I/D polymorphism in the ACE gene has been
evaluated for its role in determining the preference for physical activity. So is it
possible that, given a certain genotype I/D ACE gene, an individual could be more
prone to physical activity and consequently this would lead to a protection against
hypertension. The aim of this paper was to evaluate whether the elderly with a specific
I/D polymorphism in the ACE gene exhibit enhanced exercise capacity and whether
they are less likely to have HE. Methods: Thus, the sample consisted of 57 elderly
normotensive and 57 hypertensive patients matched for sex and age. Genotyping was
performed by polymerase chain reaction (PCR) analysis of the fragments on agarose
gel. Exercise capacity was assessed by testing the 6-minute walk (6MWT).
Hypertension was defined according to standards recommended by the World Health
Organization (WHO / ISH, 1999). The Chi-square test was used to investigate the
association between demographic characteristics, body mass index (BMI), 6MWT and
the frequency of I/D polymorphism of the ACE gene and hypertension in the elderly,
as well as to assess the genotype frequency was in Hardy-Weinberg equilibrium. The
influence of genetic polymorphism, the ability to exercise on hypertension was
assessed by analysis of odds ratio (OR) and confidence interval (CI) of 95%, obtained
by logistic regression. The significance level for all analyzes was p ≤ 0.05. Results:
The hypertensive group showed significantly higher BMI than the normotensive group,
and showed a poorer ability to exercise and frequency greater than the DD genotype
and D allele (p <0.05). The results of the analysis of genetic polymorphism for the
presence of alleles in elderly showed a higher frequency than the DD genotype

(49.1%), followed by ID (42.1%) and II (8.8%). The results of logistic regression
showed that the presence of the DD genotype (p = 0.006), obesity (p = 0.05) and
worse exercise capacity (p =0.001 indicate a greater chance of developing
hypertension elderly. The elderly patients with DD genotype had a higher chance of
37% to be hypertensive (OR = 1.37, 95%CI:1.09-1.41). The elderly obese had a
higher chance of 16% to be hypertensive compared to older people without obesity
(OR=1,16, 95%CI: 1.01-1.33), as well as individuals with poor exercise capacity were
1.24 (95%CI:1.09-1.41) times more likely to be hypertensive than those with better
exercise capacity. Observed a significant association between hypertension and
female gender carrier DD genotype (OR = 1.47, 95%CI: 1.05-2.06; p=0.025) was
confirmed by the multivariate analysis. Conclusions: Elderly physically independent
carriers of the DD genotype showed a lower exercise capacity and consequently a
greater chance of increased hypertension. The presence of the DD genotype may
have contributed to the hypertension especially in the female gender.
Keywords: RS4646994. Hypertension. Genetic polymorphism. Angiotensin converting
enzyme. Elderly. Exercise capacity.

LISTA DE ILUSTRAÇÕES
Figura 1 – Sistema renina-angiotensina ................................................................. 16
Figura 2 – Gel de eletroforese evidenciando as bandas de fragmentos .................. 28
Figura 3 – Distribuição genotípica de acordo com gênero e hipertensão ................ 33

LISTA DE TABELAS
Tabela 1 – Características demográficas, índice de massa corpórea, capacidade de
exercício, distribuição genotípica e frequência alélica em hipertensos e
normotensos...............................................................................................................31
Tabela 2 – Regressão logística simples e múltipla das variáveis exploratórias .... .32

LISTA DE ABREVIATURAS E SIGLAS
6MWT Six minute walk test
ACE Angiotensin converting enzyme
Ang II Angiotensina II
Ang II Angiotensin II
BMI Body mass index
ECA Enzima conversora de angiotensina
EH Essential hypertension
GH Growth hormone
GH Hormônio do crescimento
HAS Hipertensão arterial sistêmica
HE Hipertensão essencial
I/D Insertion/deletion
I/D Inserção/deleção
IGF-1 Fator de crescimento semelhante a insulina
IGFs Insulin-like growth factor
IMC Índice de massa corporal
PCR Polymerase chain reaction
PCR Reação em cadeia da polimerase
RAS Renin-angiotensin system
SAH Systemic arterial hypertension
SRA Sistema renina-angiotensina
TC6 Teste de caminhada de seis minutos
VO2 max Consumo máximo de oxigênio
VO2 max Maximal oxygen uptake
SUMÁRIO
1 INTRODUÇÃO ....................................................................................................... 12
2 REVISÃO DE LITERATURA - CONTEXTUALIZAÇÃO ........................................ 14
2.1 EPIDEMIOLOGIA DA HIPERTENSÃO ........................................................................... 14
2.2 FUNÇÃO DA ECA NO CONTROLE DA PRESSÃO ARTERIAL....................... ..................... 15
2.3 ESTUDOS DE ASSOCIAÇÃO ENTRE A ECA E PRESSÃO ARTERIAL ................................. 17
2.4 RELAÇÃO DO POLIMORFISMO NO GENE DA ECA COM ATIVIDADE FÍSICA ....................... 18
ARTIGO................................................................................................................................ 22
CONCLUSÃO GERAL .............................................................................................. 40
REFERÊNCIAS ......................................................................................................... 41
ANEXOS .................................................................................................................. 45
ANEXO A – Parecer de aprovação do Comitê de Ética em Pesquisa ..................... 46
ANEXO B – Termo de Consentimento Livre e Esclarecido ...................................... 47
ANEXO C – Normas de formatação do periódico Archives of Gerontology and Geriatrics ..................................................................................................................49
12
1 INTRODUÇÃO
A hipertensão essencial (HE) é um dos principais fatores de risco
cardiovascular e o principal fator de risco atribuído para mortalidade no mundo1. A
enzima conversora de angiotensina (ECA) participa tanto da conversão da
angiotensina I em angiotensina II (Ang II), como da inativação da bradicinina. A Ang
II exerce suas funções localmente em tecidos onde é produzida (rins, vasos,
coração, etc.) e sistemicamente mantendo a homeostasia cardiovascular, atuando
sobre receptores específicos2.
Fisiopatologicamente a hipertensão arterial primária ou essencial é um
fenótipo final extremamente complexo, influenciado pelo meio ambiente e por
múltiplos sistemas regulatórios redundantes (fenótipos intermediários). Portanto,
potencialmente, muitos genes devem influenciar no débito cardíaco versus
resistência vascular periférica, e o equilíbrio entre os fatores vasodilatadores e
vasoconstritores3,4.
O sistema renina-angiotensina (SRA) apresenta alguns componentes que
desempenham papéis importantes em condições normais na regulação da pressão
arterial, e alterações nesse sistema levam à progressão de
processos fisiopatológicos e doenças cardiovasculares, assim como a
hipertensão5.
Existem vários genes alvos no SRA, sendo um dos mais estudados o
polimorfismo Alu I/D (inserção/deleção) no gene da ECA, uma vez que essa
enzima é responsável por efeitos vasoconstritores. Logo, variações genéticas
podem resultar em aumento ou diminuição da concentração sérica e tecidual desta
enzima6. Estudos tem investigado a associação deste polimorfismo com o fenótipo
cardiovascular. Bae et al. (2007)7 investigaram a interação entre o polimorfismo I/D
no gene da ECA, o polimorfismo C825T GNB3 (gene da proteína G) e hipertensão
em uma população Koreana. O estudo do tipo caso controle foi constituído por 688
hipertensos e 924 normotensos. Os autores encontraram associação significativa
entre os genes e a hipertensão essencial (OR= 1,49; IC 95%:1,12-1,99; p= 0,006).
Vale ressaltar que, o treinamento físico é uma estratégia terapêutica aceita
no tratamento de indivíduos com hipertensão moderada. As interações entre o
estado de atividade física, bem como o da pressão arterial, e o risco cardiovascular

13
enfatizam a importância de compreender a relação entre o genótipo e a atividade
física em pacientes hipertensos8. Tem sido investigada a relação entre o
polimorfismo no gene da ECA e o seu papel na preferência pela atividade
física9,10,11,8. Há evidências demonstrando que o SRA também atua no tecido
muscular-esquelético como uma proteína de membrana12.
Dados na literatura inferem que indivíduos portadores do alelo I do gene da
ECA tem maior eficiência contrátil podendo beneficiar atletas de longa duração
(endurance) e os que portam o alelo D apresentam maior capacidade hipertrófica
auxiliando atletas que exigem força e potência durante as provas13. Myerson et
al.14 pesquisaram uma população de 91 corredores britânicos de padrão olímpico e
observaram uma associação significativa entre o alelo I do gene da ECA e provas
de resistência (p= 0,009).
Atualmente já está bem estabelecido que a falta de atividade física
constitua um fator de risco independente e importante para o surgimento da
hipertensão. A atividade física é sugerida como sendo um dos estilos de vida . No
entanto, o controle da pressão arterial varia muito em pacientes que receberam
intervenção de exercício, sugerindo a presença e influência das variações
genéticas16.
Considerando a falta de evidências entre a interação do polimorfismo I/D
no gene da ECA e capacidade funcional em idosos hipertensos fisicamente
independentes e, ainda, por não existir até o momento relatos na literatura
brasileira que tenham investigado a associação entre o polimorfismo I/D no gene
da ECA (RS 4646994), capacidade de exercício e hipertensão essencial em idosos
fisicamente independentes, o objetivo do presente estudo foi avaliar a associação
entre o polimorfismo genético, capacidade de exercício e a hipertensão em idosos
fisicamente independentes.

14
2 REVISÃO DE LITERATURA
2.1 Epidemiologia da hipertensão
A Organização Mundial da Saúde estima que 600 milhões de pessoas no
mundo sejam acometidas pela HAS (Hipertensão arterial sistêmica). No continente
americano são cerca de 140 milhões de pessoas, metade das quais desconhece
ser portador da doença por não apresentar sintomas e não procurar serviços de
saúde. Na América Latina e no Caribe, estima-se que de 8% a 30% da população
sejam hipertensas, respectivamente17.
As alterações dos níveis pressóricos são decorrentes dos fatores genéticos
e ambientais. Os fatores ambientais atuam nos indivíduos suscetíveis, por
exemplo, hábitos de estilo de vida, como o excesso na ingestão de sal. Os fatores
genéticos e ambientais são igualmente importantes na determinação da pressão
arterial ao longo da vida, pois a relação entre fatores genéticos e ambientais inicia-
se precocemente, ainda no período pré-natal18,5.
A elevação da pressão arterial é um sinal de manifestação de doença
específica na hipertensão arterial secundária, que corresponde a 5% dos casos.
Nos casos de hipertensão primária ou essencial, é sinal de que um conjunto de
fatores compromete o sistema cardiovascular e responde pelos demais 95% dos
casos de HAS. Nesses casos, sua manifestação e gravidade são influenciadas por
fatores extrínsecos como quantidade de sal na dieta, padrão de atividade física,
peso corporal, tabagismo e comorbidades, como o diabetes mellitus16. Assim, a
abordagem desse problema de saúde exige ações de promoção à saúde,
prevenção de agravos e cuidado do estado clínico13. Consensos e diretrizes
norteando essas iniciativas estão amplamente estabelecidas e divulgadas19.
A HAS é um problema de saúde pública que acomete aproximadamente
22,3% a 43,9% da população brasileira urbana e adulta e mais da metade dos
idosos em todo o mundo20. A HAS é considerada um dos fatores de risco para o
desenvolvimento de doenças cardiovasculares, o que explica 40% das mortes por
acidente vascular encefálico e 25% das mortes por doenças coronarianas. Por ser
muitas vezes assintomática, cerca de 40% a 83% dos pacientes desconhecem
possuir o problema de saúde20.
15
2.2 FUNÇÃO DA ECA NO CONTROLE DA PRESSÃO ARTERIAL
Usando os conhecimentos dos processos envolvidos na regulação da
pressão arterial, vários genes têm sido reconhecidos como candidatos na
contribuição para a hipertensão. Os polimorfismos nos genes que codificam a ECA
(polimorfismo Alu I/D, rs4646994),21,22 angiotensinogênio (AGT M/T235 rs 699,
AGT T/M174)23,24 e o receptor AT1 da AngII (AGTR1 A1166C, rs5186)25,26 foram
identificados como fatores genéticos importantes na patogênese da HAS e
relacionados com eventos cardiovasculares.
O SRA apresenta alguns componentes que desempenham papéis
importantes em condições normais na regulação da pressão arterial, e, alterações
nesse sistema levam à progressão de processos fisiopatológicos e doenças
cardiovasculares5.
O SRA desempenha importante função no controle e homeostasia do
sistema circulatório humano27. A cascata bioquímica se inicia com a liberação da
enzima renina produzida pelas células renais justaglomerulares, um tipo
modificado de célula muscular lisa localizada nas arteríolas aferentes. A renina
converte o angiotensinogênio, liberando um peptídeo de 10 aminoácidos, a
angiotensina I, que possui propriedades vasoconstritoras leves. A angiotensina I é
clivada, por ação da ECA, em um peptídeo de oito aminoácidos, a AngII que
apresenta capacidade vasoconstritora bem mais importante28.
Uma representação esquemática da cascata bioquímica do SRA pode ser
observada na Figura 1.

16
Figura 1 – Representação esquemática demonstrando as moléculas envolvidas na
cascata bioquímica do SRA. Terry et al29
., 2010.
Essa resposta fisiológica é mediada predominantemente por ação em
receptores específicos para Ang II (receptores AT1 e AT2) localizados na superfície
celular25. Além da sua ação vasoconstritora, a Ang II provoca aumento da pressão
arterial pela retenção de sais e água nos túbulos renais, secundária à ação da
aldosterona liberada pelas glândulas supra-renais27,28.
Em adição, a literatura demonstra a existência de SRA nos tecidos
cardíaco30,31, adiposo32 e muscular esquelético33. Outra função determinante da
ECA concentra-se na hidrólise da bradicinina pela remoção de um dipeptídeo da
região C terminal34, o que provoca sua desativação. A bradicinina é um peptídeo
de ação vasodilatadora e inibidora do crescimento celular e promove seu efeito por
ação em receptores específicos B1R e B2R35. Vale ressaltar que o gene da ECA
(21 Kbp) está localizado no cromossomo 17 q23 e é composto por 26 éxons34.
17
2.3 ESTUDOS DE ASSOCIAÇÃO ENTRE A ECA E PRESSÃO ARTERIAL
A grande parte dos estudos é discordante em relação à associação entre o
polimorfismo I/D no gene da ECA e hipertensão arterial. O’Donnell et al.36
analisaram 3095 indivíduos e encontraram associação significativa com
hipertensão diastólica apenas no gênero masculino (OR=1,59; IC95%:1,13-2,23;
p= 0,02). Sakuma et al.37 investigaram a associação entre hipertensão e o
polimorfismo no gene da ECA em 184 indivíduos afrodescendentes de uma região
do Mato Grosso. Os autores observaram a relação entre o polimorfismo e
hipertensão em indivíduos acima de 40 anos (OR= 6,71; IC 95%:3,13-14,43;
p=0,001), e para aqueles com sobrepeso (OR= 3,39; IC 95%:1,48-7,74; p=0,001),
já em mulheres não houve associação significativa (p= 0,525).
Em contrapartida, outros estudos falharam em demonstrar essa
associação. Sagnella et al.38 estudaram 1577 indivíduos e não encontraram
associação entre o polimorfismo no gene da ECA e hipertensão, porém quando foi
estratificado por gênero, foi observado que as mulheres afrodescendentes
apresentaram um risco de 2,54 mais chances de desenvolverem hipertensão em
relação ao gênero masculino (OR= 2,54, IC 95%:1,38-4,65, p= 0,003).
Ned et al.39 investigaram possíveis associações entre o polimorfismo I/D no
gene da ECA e hipertensão. A amostra foi composta por 5561 participantes com
idade ≥ 20 anos. Os autores não encontraram associação significativa entre o alelo
desfavorável D e hipertensão em mulheres no grupo de origem mexicana (OR=
1,52, IC95%: 0,61-1,28; p= 0,05).
O primeiro estudo envolvendo idosos foi publicado em 1994 por Morris et
al. 40. Foram avaliados 118 indivíduos casos e 196 controles. A frequência
genotípica nesse estudo foi de 19,4% (DD), 68,1% (DI) e 12,1% (II). Não foi
encontrada associação entre o polimorfismo no gene da ECA e hipertensão.
Em 2004, Inácio et al.41, investigaram 210 indivíduos nas diversas regiões
do Brasil e constataram que a frequência alélica na população brasileira, em geral,
foi de 0,39 e 0,61 para os alelos I e D, respectivamente, semelhante a outras
populações. Contudo, houve pequena variabilidade genotípica entre as regiões
brasileiras, com variações principalmente entre os homozigotos II e DD, tendo
como frequências genotípicas médias II= 0.20, ID= 0,43 e DD= 0,37, exceto para a
região Sul, que foi uma variação genotípica significativamente diferente das
18
demais, com tendência ao aumento do genótipo DD (0,54) e diminuição do
heterozigoto (0,24), provavelmente devido à diferente composição étnica.
Almada et al. 42 conduziram um estudo transversal no qual foram avaliados
241 indivíduos atendidos no Serviço de Geriatria do Hospital Santa Casa de
Misericórdia de Vitória. A frequência genotípica foi de: 20,33% DD; 68,41% DI e
12,86% II. Os autores não encontraram associação significativa entre o
polimorfismo no gene da ECA e o desenvolvimento de hipertensão na população
estudada (p= 0,34).
2.4 RELAÇÃO ENTRE O POLIMORFISMO NO GENE DA ECA E ATIVIDADE FÍSICA
O treinamento físico é responsável por alterações fisiológicas do sistema
cardiovascular e do metabolismo muscular tanto em repouso como durante o
exercício físico submáximo e o exercício físico máximo43. Dentre as adaptações
cardiovasculares, destacam-se a marcante redução da frequência cardíaca de
repouso e o aumento do volume sistólico, e, consequentemente, a manutenção do
débito cardíaco de repouso43.
Além das adaptações cardiovasculares gerando maior capacidade de
oferta de oxigênio para os músculos, o treinamento físico promove melhorias
periféricas que proporcionam aumento da extração de oxigênio pelo músculo
esquelético em atividade, tais como aumento da atividade das enzimas do
metabolismo oxidativo44, melhora da capilarização muscular45, aumento da
condutância vascular sistêmica46, e aumento da perfusão sanguínea periférica47.
O treinamento físico aeróbio não melhora apenas o consumo máximo de
oxigênio (VO2 max), otimiza ainda os mecanismos de produção de energia aeróbia,
como menor utilização de carboidratos, aumento da oxidação de gorduras e menor
concentração de lactato sanguíneo48. As respostas adaptativas ao treinamento
físico e, consequentemente, a determinação do rendimento esportivo, podem ser
reguladas em grande parte pela variação da expressão de genes49.
A utilização das técnicas de biologia molecular, desenvolvidas nos últimos
50 anos a partir da descoberta da estrutura do DNA por Watson e Crick50, além de
permitir o avanço científico no entendimento da influência genética sobre os

19
mecanismos envolvidos em diversas funções celulares, passou a contribuir
significantemente para o estudo das respostas fisiológicas desencadeadas pelo
treinamento físico.
O nível de atividade física habitual pode ser explicado por fatores
ambientais e psicossociais51, assim como a influência genética também pode
contribuir para a propensão do indivíduo para ser ativo fisicamente52,53,54,55. O
polimorfismo no gene da ECA, em particular, tem sido investigado quanto ao seu
papel em determinar a aptidão por atividade física9,54,55,8. Assim, a associação da
genética com atividade física vem sendo objeto de estudo em grandes centros de
pesquisas do esporte56. O genótipo de inserção é associado à baixa produção da
ECA tanto sistêmica como local, o que leva à diminuição da atividade do SRA. O
genótipo ID está relacionado à moderada produção da ECA, e o genótipo de
deleção está associado ao grande aumento da ECA circulante e local, o que
confere maior atividade do SRA5. Estudos têm demonstrado a relação entre o
polimorfismo no gene da ECA e o rendimento esportivo em diferentes modalidades
esportivas57.
Williams et al.58 avaliaram 58 indivíduos saudáveis do gênero masculino,
sendo 35 para o genótipo II e 23 para o genótipo DD. A eficiência contrátil
muscular foi medida antes e após 11 semanas de um programa de treinamento
físico aeróbico. A energia utilizada por unidade de potência não mostrou ser
diferente entre os alelos I e D (24,5% e 24,9%, respectivamente). No período pós-
treinamento, no entanto, essa variável aumentou significativamente entre os
indivíduos com alelo I. Essa diferença representa aumento na eficiência, relativa ao
período pré-treinamento, de 8,62% para o alelo I e 0,39% para o alelo D. Os
autores desconhecem os mecanismos pelos quais o alelo I estaria potencializando
a eficiência mecânica em indivíduos treinados. No entanto, mostram duas
possíveis explicações: 1) a baixa atividade enzimática da ECA no genótipo II
poderia melhorar a função contrátil na musculatura cardíaca e esquelética via
melhora na eficiência da oxidação mitocondrial, fator este mediado pelo aumento
local na concentração de óxido nítrico59, e 2) a maior eficiência muscular poderia
estar relacionada à constituição das fibras musculares, com o genótipo II
apresentando maior percentual de fibras do tipo I (fibras de contração lenta), que
são mais eficientes do que as fibras de contração rápida (tipo II) quando a
atividade contrátil muscular é realizada em baixa velocidade.

20
Zhang et al. 60 corroboraram para uma das hipóteses de Williams et al58.
Foi realizada a biópsia do músculo vasto lateral de 41 indivíduos sedentários,
sendo observada associação entre os genótipos da ECA e a distribuição
percentual de fibras do tipo I (contração lenta), IIa (contração rápida) e IIb
(contração rápida). Indivíduos com alelo I quando comparados com alelo D
apresentaram maior média percentual de fibras do tipo I (fibras adaptadas para
exercícios aeróbicos) e menor média percentual de fibras do tipo IIb. Não houve
diferença estatisticamente significante entre os genótipos para os valores de média
percentual para as fibras do tipo IIa. Embora não esteja claro o mecanismo pelo
qual o gene da ECA determina a distribuição dos diferentes tipos de fibras nos
músculos, esses resultados vêm corroborar estudos que mostraram associação do
alelo I com alta performance em atletas de resistência.
É bem aceito na literatura que os dois alelos funcionais I/D no gene da
ECA diferem em seus efeitos sobre a capacidade atlética61, com o alelo I
favorecendo modalidades de resistência, e o alelo D favorecendo modalidades de
força muscular62.
A manutenção e melhoria da função muscular são importantes para uma
boa capacidade de exercício, além de melhorar a capacidade funcional e retardar a
progressão da sarcopenia em idosos63. Sarcopenia é o declínio da massa
muscular e sua função relacionada à idade64, e se reflete no aumento da
mortalidade, pois está relacionada com as incapacidades funcionais e risco de
quedas, quando associada a outras comorbidades crônico-degenerativas como
diabetes, obesidade, HAS, e síndrome metabólica65. O mecanismo da sarcopenia
envolve o eixo do hormônio do crescimento (GH) e do fator de crescimento
semelhante à insulina, (IGF-1), os quais são afetados pela Ang II66. O aumento dos
níveis de AngII pode contribuir para o desenvolvimento da sarcopenia, quer
acelerando a degradação de proteínas através da via proteolítica ou reduzindo a
síntese de proteínas através da inibição do GH/IGF-1 em músculos esqueléticos67.
A atividade cronicamente baixa persistente da ECA, causada por
medicamentos inibidores da ECA, impedem a queda da força muscular relacionada
à idade. O alelo I promove uma menor atividade da enzima, o que pode afetar a
mudança da força muscular relacionada à idade68.
Em 2012, Hyeon et al.63 investigaram a associação do polimorfismo da
ECA com a fatigabilidade muscular em idosos coreanos. Para isso utilizaram os
21
valores de índice de massa corporal (IMC) obtidos por espectrometria de massa, e
para medir a fadiga muscular utilizaram dados de eletromiografia dinâmica. A
atividade enzimática foi significativamente maior para o alelo D do que para o alelo
I (p˂0,05) e o alelo I mostrou significativamente maior resistência à fadiga muscular
do que o alelo D (p˂0,05). No entanto, a obesidade medida pelo IMC não mostrou
associação com o polimorfismo da ECA (p= 0,392).
O estudo da efetividade do exercício no tratamento da hipertensão ainda
deixa muitas lacunas. Embora seja bem estabelecido que o treinamento
cardiovascular é o modo mais eficaz de exercício na prevenção e no tratamento da
hipertensão, nem todos os pacientes hipertensos respondem a esse treinamento.
Diferenças em relação à resposta ao exercício podem ser em função da
variabilidade genética, processos fisiopatologicos diferentes, e prescrição
inconsistente de exercício. Já existem ferramentas para investigar a dose ótima de
exercício para hipertensos leves e não respondedores aos outros tratamentos.
Observação da resposta ambulatorial da pressão arterial após ajustes na execução
do exercício pode ser um meio eficaz para encontrar a dose de exercício que pode
ser mais eficaz para uma população específica69.
Winnicki et al.8 testaram a hipótese de que a promoção de exercícios
aeróbicos em hipertensos leves não seria adequada para os indivíduos
homozigotos DD do polimorfismo I/D no gene da ECA, e resultaria na tendência ao
sedentarismo entre esses sujeitos em comparação aos homozigotos II do mesmo
polimorfismo. Os autores encontraram que o estilo de vida sedentário foi mais
comum entre os hipertensos homozigotos DD do que nos homozigotos II. Os
resultados deste estudo sugerem que o polimorfismo I/D no gene da ECA pode ser
fator genético específico associado ao nível de atividade física em indivíduos
hipertensos leves e limítrofes. Os achados de Wong et al. 70, em 2012 corroboram
estes resultados. Estes pesquisadores identificaram que o genótipo da ECA foi
idependentemente associado com o nível de atividade física. Os indivíduos com
genótipos DD ou ID relataram nível de atividade física insuficiente ou baixo quando
comparados aos indivíduos com o genótipo II (OR= 6,88; 95%IC:2,26-20,94).
Considerando a falta de evidências entre a interação do polimorfismo I/D
no gene da ECA e capacidade funcional em idosos hipertensos fisicamente
independentes e, ainda, por não existir até o momento relatos na literatura
brasileira que a tenha investigado, o objetivo do presente estudo foi avaliar a

22
associação entre o polimorfismo genético, a capacidade de exercício e a
hipertensão em idosos fisicamente independentes.
23
ARTIGO
ASSOCIATION OF HYPERTENSION WITH ACE I/D POLYMORPHISM
(RS4646994) AND EXERCISE CAPACITY IN BRAZILIAN ELDERLY: A CASE
CONTROL STUDY.
(A ser submetido ao periódico Archives of Gerontology and Geriatrics- Qualis B1)
Cleber Veloso Carvalhoa,b
, Vanessa Suziane Probsta,c
, Sandra Mara Macield, Denilson
Texieirac, Regina Célia Poli-Frederico
a,b,*
aMaster Program in Rehabilitation Sciences UEL-UNOPAR, Av. Paris 675 Jd Piza, CEP
86041-140. Cx. P. 401, Londrina, PR, Brazil.
bLaboratory of Molecular Biology, Universidade Norte do Paraná (UNOPAR). Av. Paris 675,
Jd Piza, CEP 86041-140. Cx. P. 401, Londrina, PR, Brazil.
c Centre of Research in Health Sciences, Universidade Norte do Paraná (UNOPAR). Av. Paris
675, Jd Piza, CEP 86041-140. Cx. P. 401, Londrina, PR, Brazil.
dDepartment of Pediatric Dentistry, Dental School, Universidade Estadual de Maingá (UEM),
Maringá – Paraná, Brazil .
Short Title: Hypertension and ACE I/D polymorphism.
Key words: rs4646994; hypertension; genetic polymorphism; ACE; exercise capacity,
elderly.
*Correspondence author at: Regina Célia Poli-Frederico
Laboratory of Molecular Biology, University Norte do Paraná (UNOPAR), Av. Paris 675, Jd
Piza, CEP 86041-140. Cx. P. 401, Londrina, PR, Brazil. Phone: +55-43-3371-7820 Fax: +55-
43-3371-7741
E-mail address: [email protected]; [email protected]
Declaration of Interests: There are no conflicts of interest in this paper, stated by each
author.

24
Abstract
Background: The renin-angiotensin system (RAS) plays a fundamental role in regulating
blood pressure, and polymorphisms in the genes encoding angiotensinogen, angiotensin II and
angiotensin converting enzyme (ACE) inhibitor may influence the risk of hypertension. A
ACE catalyzes the conversion of angiotensin I to angiotensin II (vasoconstrictor) and
performs the inactivation of bradykinin (vasodilator). The ACE gene is characterized by the
insertion (I) or deletion (D) of an Alu repeat sequence in intron 16. This polymorphism (RS
4646994) insertion/deletion (I/D) ACE results in changes in plasma levels of the enzyme and
thus have a fundamental role in the homeostasis of blood pressure. In addition, it is known
that physical inactivity is also a risk factor for cardiovascular disease, including hypertension.
The level of physical activity can be explained by psychosocial and environmental factors, but
genetic influence should also be taken into account in the individual's propensity to be
physically active. Thus, the aim of this study was to assess whether the influences of gender,
age, body mass index (BMI), and exercise capacity on hypertension are homogenous among
genotypes I/D in ACE. Methods: The study sample consisted of 57 health elderly and 57
hypertensive elderly. Genotyping for insertion/deletion of ACE was performed by polymerase
chain reaction (PCR). The influence of parameters on the risk of hypertension among
physically independent Brazilian elderly was assessed by analysis of logistic regression. The
significance level for all analyses was p ≤ 0.05. Results: After adjustment for age, sex, body
mass index, exercise capacity, polymorphism I/D ACE, the elderly with the ACE DD
genotype were 1.37 (95%CI:1.09-1.71) more likely to be hypertensive than carriers of the
allele I (p=0.006). The hypertensive group exhibited a significantly higher BMI than the
normotensive group, as well as elderly with impaired exercise capacity were likely to be
hypertensive than those with more preserved exercise capacity. In addition, the association
between hypertension and DD genotype in women but not in men was confirmed by the
multivariate analysis. Conclusions: Our data provide evidence that physically independent
elderly carriers of the DD genotype showed a impaired exercise capacity and consequently an
increased risk of hypertension. BMI was also associated with hypertension in this population.
Additionally, the presence of the DD genotype may have contributed to the disease
hypertension especially in the female gender.
25
Introduction
Essential hypertension (EH) is a common complex disease caused by both genetic and
environmental factors (Lufit, 2004). Although the precise aetiology of EH remains unclear,
accumulating evidence has suggested that genetic susceptibility is a important factor for the
development of EH (Jiang et al., 2009). Renin-angiotensin system (RAS) genes encoding for
angiotensinogen, angiotensin type 1 receptor and angiotensin-converting enzyme (ACE) have
been widely investigated in different ethnic populations (Barbalic et al., 2006; Bae et al., 2007
Province et al., 2000; Sugimoto et al., 2004; Velez et al., 2006).
ACE insertion/deletion (I/D) polymorphism has been the major target for genetic
investigations of hypertension (Corvol et al., 1999; Lifton, 1995; Matsubara, 2000;
Matsubara et al., 2002). ACE, which generates angiotensin II and degrades bradykinin, is
located on chromosome 17q23 (Mattei et al., 1989), being encoded by 21 kb, 26 exon gene.
An I/D polymorphism of the ACE gene consists of the absence and presence of a 287 bp
DNA fragment located near the 3’ end of intron 16 (Rigat et al., 1990). About half of the
interindividual variations in plasma ACE levels are due to the presence of an I/D
polymorphism. Individuals who are homozygous for the deletion allele (DD) have serum
ACE levels higher than those who are homozygous for the insertion allele (II) (Cambien et al.,
1988), and therefore it has been hypothesized that ACE I/D polymorphism is associated with
blood pressure level or the onset of hypertension (Corvol et al., 1999; Lifton, 1995;
Matsubara, 2000; Matsubara et al., 2002).
Despite universal recognition that blood pressure is influenced by interaction between
the effects of many genetic and environmental factors, the ACE I/D polymorphism and effects
of other genetics and environmental factors has received little attention (Turner et al., 1999).
Although Staessen et al. (1997) found that the D-allele of ACE I/D polymorphism was not
associated with hypertension, but however others studies demonstrated a significant
association between this polymorphism and hypertension in male subjects (Higaki et al.,
2000; O’Donnell et al., 1998).
In addition, accumulated evidence suggests the importance of obesity prevention to
protect against age-and lifestyle-related diseases, such as hypertension (Nakamura et al.,
2007; Schjerve et al., 1990), as well as, regular physical activity has protective effects for
several chronic diseases, including hypertension, whereas low levels of physical fitness are
associated with increased all-causes mortality rates (Pate et al., 1995). Others reports
additionally suggest that the ACE I/D may be associated to the anabolic response and the left
26
ventricular growth induced by physical training (Montgomery et al., 1998; Williams et al.,
2000), maximal oxygen consumption (Hagberg et al., 1998), and elite athletic performance
(Alvarez et al., 2000; Myerson et al., 1999). Thus it could be possible that, given an ACE I/D
genotype, subjects might be more likely to become physically active and, consequently this in
turn would lead to protection against hypertension. Hence and, considering that there are few
reports in the literature regarding polymorphism genetic and exercise capacity in older adults,
the aim of this study were to evaluate the association of the ACE I/D polymorphism with
functional exercise capacity and history of hypertension in physically independent elderly.
Material and methods
Subjects
For this cross-sectional study, the convenience sample consisted of elderly who
participated on an interdisciplinary project (EELO Project – study on aging and longevity),
which aimed was to perform an epidemiological study of socio-demographic factors and
indicators of health conditions in the elderly in Londrina, a city of Northern Paraná, Brazil.
Information could be found at http://www2.unopar.br/sites/eelo.
The study included individuals aged ≥ 60 years and paraded by gender and age,
physically independent according to the classification proposed by the Functional Status
Spirduso (levels 3 and 4) (Spirduso, 2005). A case-control study age and sex matched was
performed between 57 subjects in the hypertensive (mean age 69.2 ± 5.7) group and 57
subjects in the normotensive group (mean age 69.2 ± 5.7).
The criteria for inclusion were: age over 60 years, complete independence for daily
activities; absence of severe comorbidities that would prevent completion of the test,
including pre-diagnosed incapacitating cardiac and orthopedic diseases. Individuals with
neuro-musculo-skeletal disease and mental limitations that would impair the understanding
and performance of the tests involved in the study were excluded. All subjects agreed to
participate and signed a written informed consent. The project was approved by the Ethics
Committee of the UNOPAR (PP0253/11).
Obesity was diagnosed on the basis of the most commonly used definitions,
established by the World Health Organization (WHO) in 1997 and published in 2000, that
defines the body mass index (BMI) of obesity as being 30 or greater (WHO, 2000). BMI was
determinate with the following formula: body mass divided by height squared (Kg/m2). The
blood pressure was obtained in the right arm after the participant sat quietly for ≥ 5 minutes.

27
Hypertension was diagnosed according to the diagnostic standard of hypertension set by
WHO/ISH in 1999 (systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥
90mmHg) and if these individuals reported a previous diagnosis of hypertension and if were
being treated with antihypertensive medications. Normotensives were selected from the same
population with SBP < 140 mm Hg and DBP < 90 mm Hg and the absence of hypertension
disease history.
6-Minute Walk Test (6MWT)
The 6MWT evaluates the subject’s functional exercise capacity and was performed in
accordance with the guidelines of the American Thoracic Society (2002). The analysis was
based on the percentage of values predicted according to Troosters et al (1999). The more
preserved exercise capacity group (n= 91) was composed of individuals who achieved 80% or
more of the predicted value on the 6MWT and, the impaired exercise capacity group (n= 12)
composed of individuals who achieved less than 80% of the predicted value on the 6MWT.
Importantly, 11 individuals were absent on test day, but for other analyzes there was no
prejudice.
DNA samples
Blood samples were collected at EDTA added tubes, and buffy coat was separated and
stored at -80 ºC. DNA was extracted using a commercially available kit (QIAmp DNA Blood
Midi Kit – Qiagen) according to the manufacturer's instructions.
Determination of ACE I/D polymorphism (rs4646994)
The following primer pair was used for PCR amplification of genomic DNA samples:
forward 5'CTG GAG ACC ACT CCC ATC CTT TCT3' and reverse 5'GAT GTG GCC ATC
ACA TTC GTC AGAT3' (Invitrogen, Carlsbad, CA) (Rigat et al., 1990). Amplification
reactions were carried out with 100 ng of genomic DNA in a total volume of 25 µL,
containing 10mM Tris-HCl (pH 8.3), 50mM KCl, 1 µM of each primer, 200 µM of each
dATP, dCTP, dGTP and dTTP, 1.5mM MgCl2, and 1 U Taq DNA polymerase (Invitrogen).
The reaction was incubated for 5 min at 95°C, followed by 30 cycles of 1 minute at 95°C, 1
minute at 58°C and 2 minutes at 72°C, and a final extension at 72°C for 5 min. After
amplification, 10 µL of the PCR product was analyzed by agarose gel electrophoresis (2%).
Subsequently the gel was stained with Syber-safe (Invitrogen) and the newly synthesized
fragments were visualized under ultraviolet light. The size of the PCR amplified product was

28
estimated from the electrophoretic migration of the product relative to the marker 100 bp
DNA Ladder (Invitrogen). The 190 bp deletion allele and the 490 bp insertion allele were
identified by Syber-safe (Invitrogen) staining (Figure 2).
Figure 2. Fragments of insertion (490 pb) and deletion (190 pb)
in the ACE gene; NO: negative control; PM: molecular weight
marker 100 bp.
Statistical analysis
Statistical analysis was performed with SPSS package version 15.0 (SPSS Inc.,
Chicago, IL, USA). Subjects’ characteristics were expressed as means, standard deviation
(±SD) and percentages. Differences in distributions of genotypes as well as frequencies of
alleles for the polymorphism were analyzed by Fisher exact tests and Chi-square test among
the groups. Hardy-Weinberg equilibrium was tested in each group by a chi-square test.
The association between hypertension and genotype, BMI, exercise capacity was
calculated by the Odds ratio (OR) [95% confidence intervals (CIs)]. The differences between
the groups were further analyzed through of the simple and multiple logistic regression
models with adjustment for age, gender, exercise capacity, genotypes and BMI. P-value <0.05
were considered as statistically significant.
PM A E D C B F G
I I I D
D D
29
Results
Clinical and demographic characteristics of all 114 subjects are presented in Table 1.
The hypertensive group exhibited a significantly higher BMI (p=0.027) than the normotensive
group, however there were no significant differences in age and gender between the two
groups, once the sample was matched for sex and age. It was found a significant association
between exercise capacity and hypertension. The elderly that presented impaired exercise
capacity were hypertensives, while those that had high exercise capacity were normotensive
(2= 6.58; p=0.013).
The results of the genetic polymorphism analysis showed a higher frequency of DD
genotype (49.1%), followed by ID (42.1%), and II (8.8%) genotype. The genotypic
frequencies determined in this study did not deviate from those predicted by the Hardy-
Weinberg Equilibrium (2 test; p = 0.949).
The ACE I/D polymorphism displayed significant differences in the allelic and
genotypic frequencies between hypertensive and normotensive groups (Table 1). The allele
frequencies of ACE I/D with D allele, and the DD genotype were higher in the hypertensive
group (2=5.21, p=0.042; 2= 4.82, p=0.043, respectively).
Results from simple logistic regression (Table 2) showed that the presence of DD
genotype was associated with the elderly’ hypertension experience. Elderly positive for this
genotype were more likely to have hypertension than those who were negative (OR=1.31,
95%CI:1.04-1.64; p=0.018). Body mass index was also significantly associated with the
outcome variable (OR=1.29, 95%CI:1.09-1.53; p= 0.004), as well as it was found association
between exercise capacity and hypertension. The elderly that had low exercise capacity
showed 1.27 (95%CI:1.11-1.46; p=0.005) more likely to have hypertension that those who
had higher exercise capacity. None of the other variables were significant.
In the multiple logistic regression (Table 2), the BMI (p=0.05), the 6MWT (p=0.001)
and the DD genotypes (p=0.006) remained significant, indicating that these variables were
independently related to the elderly’ hypertension experience. Elderly that presented high
BMI had 1.16 (95%CI:1.01- 1.33) times more likely to have hypertension, as well as those
that had low exercise capacity 1.24 (95%CI:1.09-1.41)and, those elderly who harbored ID and
DD genotypes had, respectively, 1.28 (95%CI:1.02-1.61) and 1.37 (95%CI:1.09-1.71) times
more likely to have hypertension than their counterparts.
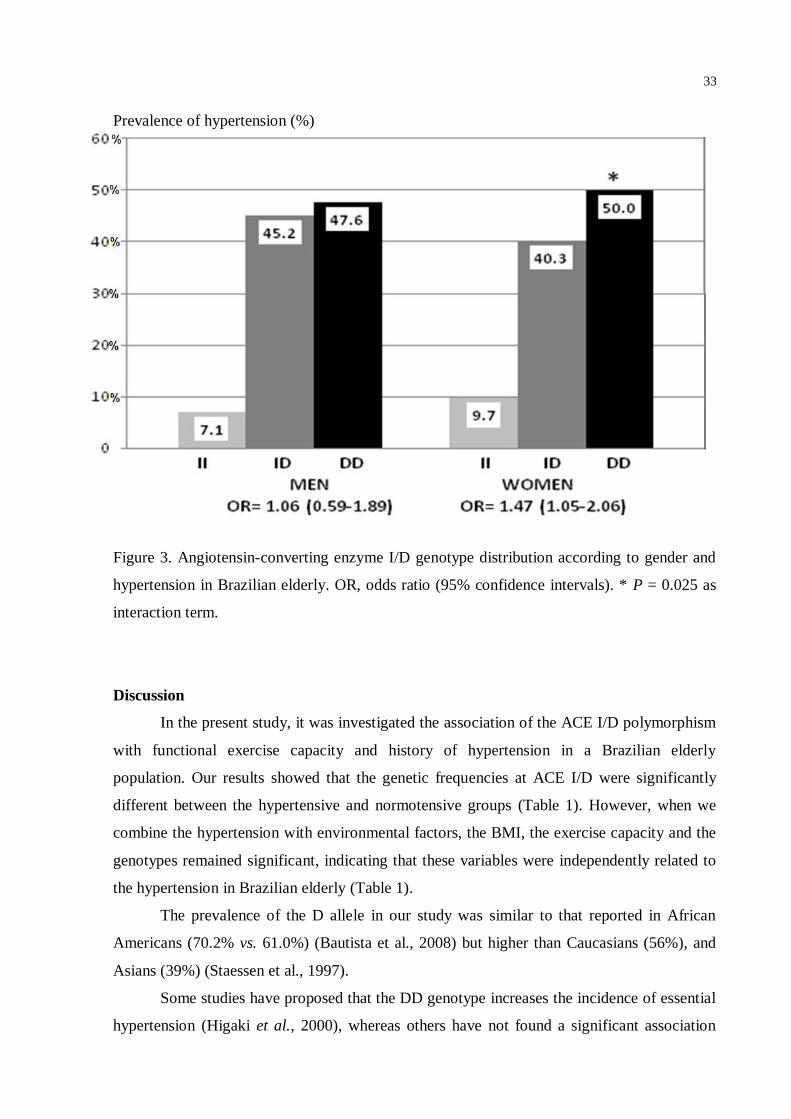
In addition, we observed an association between hypertension and the DD genotype in
women but not in men was confirmed by the multivariate analysis. In particular, although

30
there was no significant association (p=0.837) between ACE genotype and hypertension in
men (OR=1.06, 95%CI:0.56-1.89), there was a significant association (p=0.025) between this
genotype and hypertension in the women (OR= 1.47, 95%CI:1.05-2.06) (Figure 2).

31
Table 1- Demographic characteristics, body mass index, 6-Minute Walk Test and distribution
of angiotensin-converting enzyme I/D genotypic and allelic frequencies in hypertensives and
normotensives Brazilian elderly
Variables Hypertensives Normotensives P values
Gender
Male/Female
21/36
21/36
n.s.
Age (years)
60-64
65-70
≥ 71
12 (50%)
21 (50%)
24 (50%)
12 (50%)
21 (50%)
24 (50%)
n.s.
BMI (Kg/m2)
Mean±SD
Underweigth
Normal weight
Overweight
Obesity
28.56±4.51
07 (12,3)
20 (35.1)
09 (15.8)
21 (36.8)
25.78±4.02
15 (23.3)
24 (42.1)
10 (17.5)
08 (14.0)
0.027a
6MWT
High exercise capacity
Low exercise capacity
Genotypes
II
DI
DD
Alleles
I
D
40 (80.0)
10 (20.0)
02 (03.5)
23 (40.4)
32 (56.1)
27 (23.7)
87 (76.3)
51 (96.2)
02 (3.8%)
08 (14.0)
25 (43.9)
24 (42.1)
41 (35.9)
73 (64.1)
0.013b
0.043c
0.042d
BMI, body mass index; 6MWT, 6-Minute Walk Test, n.s., no significant. Statistical
significance was determined by 2 among two groups. a2=9.15.
b2=6.58.
c2=4.82.
d2=5.21.

32
Table 2. Simple and multiple logistic regressions of exploratory variables on the hypertension
history of Brazilian elderly
Exploratory Variables
Unadjusted
OR (95%CI)
P-values
Adjusted
OR (95%CI)
P-values
Gender
Female
Male
1
1.00 (0.83-1.21)
1.000
_
_
Elderly age
60-64 years
65-70 years
≥ 71 years
1
1.00 (0.78-1,28)
1.00 (0.78-1.23)
1.000
1.000
_
_
BMI
Normal weight
Underweigth
Overweight
Obesity
1
1.09 (0.91-1.30)
1.09 (0.88-1.35)
1.29 (1.09-1.53)
0.348
1.020
0.004
1
0.96 (0.80-1.15)
1.00 (0.85-1.24)
1.16 (1.01-1.33)
0.644
0.783
0.050
6MWT
High exercise capacity
Low exercise capacity
Genotypes
II
DI
DD
1
1.27 (1.11-1.46)
1
1.23 (0.93-1.51)
1.31 (1.04-1.64)
0.005
0.072
0.018
1
1.24 (1.09-1.41)
1
1.28 (1.02-1.61)
1.37 (1.09-1.71)
0.001
0.035
0.006
BMI, body mass index; 6MWT, 6-Minute Walk Test.
33
Prevalence of hypertension (%)
Figure 3. Angiotensin-converting enzyme I/D genotype distribution according to gender and
hypertension in Brazilian elderly. OR, odds ratio (95% confidence intervals). * P = 0.025 as
interaction term.
Discussion
In the present study, it was investigated the association of the ACE I/D polymorphism
with functional exercise capacity and history of hypertension in a Brazilian elderly
population. Our results showed that the genetic frequencies at ACE I/D were significantly
different between the hypertensive and normotensive groups (Table 1). However, when we
combine the hypertension with environmental factors, the BMI, the exercise capacity and the
genotypes remained significant, indicating that these variables were independently related to
the hypertension in Brazilian elderly (Table 1).
The prevalence of the D allele in our study was similar to that reported in African
Americans (70.2% vs. 61.0%) (Bautista et al., 2008) but higher than Caucasians (56%), and
Asians (39%) (Staessen et al., 1997).
Some studies have proposed that the DD genotype increases the incidence of essential
hypertension (Higaki et al., 2000), whereas others have not found a significant association

34
(Mondry et al., 2005). This inconsistent association may be due to the fact of different
ethnicity of the population groups and environmental heterogeneity (Barley et al., 1994;
O'Donnell et al., 1998; Stassen et al., 1997). Thus, further studies are needed to elucidate the
nature of this relationship.
Rasyid, Bakri and Yusuf (2012) investigated the potential association between the
ACE gene polymorphism and essential hypertension the ACE D-allele was not associated
with hypertension (p= 0.802). Negative association was also shown in Chinese population,
Italian, Greek, Japan and Indian (Ishigami et al., 1995; Martinez et al., 2000). Contradictorily,
our results showed that the elderly had statistically significant increase of 28% and 37% more
likely to develop hypertension among heterozygous and D homozygous subjects (OR=1.28;
95%CI=1.02-1.61 and OR=1.37; 95%CI=1.09-1.71, respectively), and these results are
consistent with some reports describing that there is an association of I/D polymorphism of
ACE gene with hypertension (Ali et al., 2012; Ming et al., 1996; Nakano et al., 1998; Yoshida
et al., 2000). It must be kept in mind that there is a suggestion that the association may be
stronger among Asians compared with Caucasians (Woo et al., 2012). Individuals who are
homozygous for the deletion allele (DD) have serum ACE levels higher than those who are
homozygous for the insertion allele (II) (Cambien et al., 1988), and therefore it has been
hypothesized that ACE I/D polymorphism is associated with blood pressure level or the onset
of hypertension (Corvol et al., 1999; Lifton, 1995; Matsubara, 2000; Matsubara et al., 2002).
There is lot of epidemiologic evidence to support the association between obesity and
high blood pressure (Foulds et al., 2012). Results from the present study indicated that the
elderly that were obese had 1.16 (95%CI=1.03- 1.59) times more likely to have hypertension
than their counterparts. Studies have shown that an increase in body weight (BMI) increases
body fluid volume, peripheral vascular resistance (hyperinsulinemia, cell membrane
alteration, and hyperactivity of the renin-angiotensin system leading to functional constriction
and structural hypertrophy), and cardiac output (Tuan et al., 2010).
We found a significant association between exercise capacity and hypertension, the
hypertensive elderly presented impaired exercise capacity. The general beneficial effects of
training on vascular function in hypertensive are well documented. Essential hypertension is
associated with impaired vascular function, as evidenced by a reduced vasodilatory response
to flow induced vasodilatation and acetylcholine (John and Schmieder, 2000). Exercise
interventions have, furthermore, proven successful in lowering blood pressure in individuals
with essential hypertension (McGowan et al., 2006) and several studies have shown improved
vascular function in skeletal muscle after training in hypertensive individuals (Hambrecht et

35
al., 1998; McGowan et al., 2006). It is noteworthy that in our study despite the vast majority
of elderly with more preserved exercise capacity (91) versus (12) with impaired exercise
capacity, still significant association between hypertension and capacity exercise, it shows a
tendency to increase odds ratio in a larger sample number.
In addition, the DD genotype has been linked to an increased predisposition to
cardiovascular events (Cambien and Evans, 1995). While this association remains
controversial (Keavney et al., 2000), lower physical activity levels may contribute to any
increased cardiovascular risk in the DD homozygote subjects (Winnicki et al., 2004). Two
postulates could explain how ACE genotypes influence voluntary physical activity
participation (Wong, Zhao and Koh, 2012). Earlier investigators have speculated that a higher
level of circulating ACE in DD individuals could lead to greater conversion of angiotensin I
to angiotensin II and degradation of kinins, the latter having the effect of lowering the muscle
blood flow and glucose utilization necessary for aerobic work (Dietze et al., 1980). Thus,
these cellular differences between individuals carrying the D alleles render participation in
aerobic physical activity less favorable and preferred. In addition, the observation of fewer
slow-twitch muscle fibers, which are designed for aerobic physical activity, in DD genotypes
(<20%) than in II genotypes (59%; Zhang et al., 2003) possibly leads to diminished
preference to participate in physical activity. Moreover, the responses to physical training are
shown to differ among individuals with different genotypes. Individuals carrying the I allele
were shown to have greater improvement in aerobic capacity, whereas those with the D allele
had less in response to exercise training in nonelite young individuals (Ashley et al., 2006;
Colakoglu et al., 2005; Folland et al., 2000; Jones et al., 2002). Finally, the rennin-angiotensin
system is also present in the central nervous system and may exert a central influence on
predisposition to physical activity (Dzau, 1993).
Subsequent studies demonstrated the sex-specific effects of the ACE gene (Higaki et
al., 2000; O’Donnell et al., 1998); the D allele apparently increased the risk of hypertension in
male subjects of Caucasian (O’Donnell et al., 1998) and Japanese (Higaki et al., 2000)
populations. Our present findings show a significant odds ratio for the female gender with DD
genotype (OR= 1.47; 95%CI=1.05-2.06). Our results corroborate with findings of Ned et al.
(2012) that observed a significant genotype–sex interaction among Mexican Americans, for
whom positive associations with hypertension were seen among females, but not males (OR=
1.52; 95%CI=0.61-1.28). Sagnella et al. (1999) also related the observation of a gender-
dependent association between hypertension and the D allele in African descent. There was a
significant association between the D allele and hypertension in women but not in men. These
36
authors cited that the mechanism whereby the presence of the D allele may contribute to the
expression of hypertension in women but not in men remains to be resolved.
Limitations of our study were that our results do not preclude the existence of other
gene-physical activity interactions, which important in the regulation of spontaneous physical
activity.
In conclusion, this study has provided further evidence that DD genotype in the ACE
gene, obesity, and impaired exercise capacity may act independently on prevalence of EH in
physically independent Brazilian elderly. In addition, it was observed a positive association
with hypertension among female gender with DD genotype, but not male. More studies are
necessary in order to determine correct exercise prescriptions for hypertensive DD genotype,
so as to possibly reduce inactivity, and hence hypertension, among these subjects (Winnicki et
al., 2004). Considering that little is known about the genetic basis of ACE I/D to hypertension
in Brazilian elderly, the analysis of genetic polymorphism in a sample from this population
represents important information concerning hypertension in Brazil.
Acknowledgements
The authors would like to thank the FUNADESP and UNOPAR (PP/0213/10) for
financial support.
37
References
Ali A, Alghasham A, Ismail H, Dowaidar M, Settin A. ACE I/D and eNOS E298D gene
polymorphisms in Saudi subjects with hypertension. Journal of the Renin-Angiotensin-
Aldosterone System. 2012: Oct 5.
Alvarez R, Terrados N, Ortolano R, et al. Genetic variation in the renin-angiotensin system
and athletic performance. European Journal Appllied Physiology. 2000: 82: 117–120.
American thoracic society. Statement: guidelines for the six-minute walk test. American
Journal of Respiratory and Critical Care Medicine. 2002: 166: 111-17.
Ashley EA, Kardos A, Jack ES, et al. Angiotensinconverting enzyme genotype predicts
cardiac and autonomic responses to prolonged exercise. Journal of the American College
of Cardiology. 2006: 48: 523–531.
Bae Y, Park C, Han J, et al. Interaction between GNB3 C825T and ACE I/D polymorphisms
in essential hypertension in Koreans. Journal of Human Hypertension. 2007
Feb;21(2):159-66.
Barbalić M, Skarić-Jurić T, Cambien F, et al. Gene polymorphisms of the renin-angiotensin
system and early development of hypertension. American Journal of Hypertension. 2006
Aug; 19(8):837-42.
Barley J, Blackwood A, Carter ND, et al. Angiotensin converting enzyme insertion/deletion
polymorphism: association with ethnic origin. Journal of Hypertension. 1994; 12:955–
957.
Bautista LE, Vargas CI, Oróstegui M, et al. Population-based case-control study of renin-
angiotensin system genes polymorphisms and hypertension among hispanics.
Hypertension. 2008; 31:401-408.
Cambien F, Alhenc-Gelas F, Herbeth B, et al. Familial resemblance of plasma angiotensin-
converting enzyme level: the Nancy Study. The American Journal of Human Genetics.
1988 Nov;43(5):774-80.
Colakoglu M, Cam FS, Kayitken B, et al. ACE genotype may have an effect on single versus
multiple set preferences in strength training. European Journal of Applied Physiology.
2005: 95: 20–26.
Cooper R, McFarlane-Anderson N, Bennett FI, et al. Angiotensinogen and obesity: a potential
pathway leading to hypertension. Journal of Human Hypertension. 1997; 11: 107–111.
Corvol P, Persu A, Gimenez-Roqueplo AP, et al. Seven lessons from two candidate genes in
human essential hypertension: Angiotensinogen and epithelial sodium channel.
Hypertension. 1999; 33:1324–1331.
De Moor MHM, LiuYJ, Boomsma DI, et al. Genomewide association study of exercise
behavior in Dutch and American adults. Medicine and Science in Sports and Exercise
2009; 41(10), 1887–1895.
Dietze G, Wicklmayr M, Bottger I, et al. The kallikrein-kinin system and musclemetabolism:
Biochemical aspects. Agents and Actions. 1980: 10:335–338.
Dzau VJ. 1993. Tissue renin-angiotensin system in myocardial hypertrophy and failure.
Archives of Internal Medicini. 153:937–942.
38
Folland J, Leach B, Little T, et al. Angiotensinconverting enzyme genotype affects the
response of human skeletal muscle to functional overload. Experimental Physiology.
2000: 85: 575–579.
Foulds HJ, Bredin SS, Warburton DE. The relationship between hypertension and obesity
across different ethnicities. Journal of Hypertension. 2012;30:359–367.
Fuentes RM, Perola M, Nissinen A, et al. ACE gene and physical activity, blood pressure, and
hypertension: A population study in Finland. Journal of Applied Physiology 2002; 92(6),
2508–2512.
Hagberg JM, Ferrell RE, McCole SD, et al. VO2 max is associated with ACE genotype in
postmenopausal women. Journal of Applied Physiology 1998; 85(5), 1842–1846.
Hambrecht R, Fiehn E, Weigl C, Gielen S, Hamann C, Kaiser R, Yu J, Adams V, Niebauer J,
Schuler G. Regular physical exercise corrects endothelial dysfunction and improves
exercise capacity in patients with chronic heart failure. Circulation. 1998;98:2709 –2715.
Higaki J, Baba S, Katsuya T, et al. Deletion allele of angiotensin-converting enzyme gene
increases risk of essential hypertension in Japanese men. Circulation. 2000; 101:2060–
2065.
Ishigami T, Iwanoto T, Tamura K, et al. Angiotensin I converting enzyme (ACE) gene
polymorphism and essential hypertension in Japan. American Journal of Hypertension.
1995:8;95-7.
Jiang X, Sheng H, Li J, Xun P, et al. Association between renin-angiotensin system gene
polymorphism and essential hypertension: a community-based study. Journal Human of
Hypertension. 2009 Mar; 23(3):176-81.
John S, Schmieder RE. Impaired endothelial function in arterial hypertension and
hypercholesterolemia: potential mechanisms and differences. Jounal of Hypertension.
2000;18:363–374.
Jones A, Montgomery HE, & Woods DR. Human performance: A role for the ACE genotype?
Exercise and Sport Sciences Reviews. 2002: 30: 184–190.
Keavney B, McKenzie C, Parish S, et al. Large-scale test of hypothesised associations
between the angiotensin-converting-enzyme insertion/deletion polymorphism and
myocardial infarction in about 5000 cases and 6000 controls. International Studies of
Infarct Survival (ISIS) Collaborators. Lancet. 2000: 355:434–442.
Kramer H, Wu X, Kan D, et al. Angiotensin-converting enzyme gene polymorphisms and
obesity: an examination of three black populations. Obesity Research. 2005; 13: 823–
828.
Lifton RP. Genetic determinants of human hypertension. Proceedings of the National cademy
os Sciences of the United States os America. 1995; 92:9545–9551.
Luffit FC. Geneticism of essential hypertension. Hypertension. 2004; 43: 1155-1159.
Martinez E, Puras A, Escribano J, et al. Angiotensin-converting enzyme (ACE) gene
polymorphisms, serum ACE activity and blood pressure in a Spanish Mediterranean
population. Journal Human of Hypertension. 2000:14;131-5.
Matsubara M, Ohkubo T, Michimata M, et al. Japanese individuals do not harbor the T594M
mutation but do have the P592S mutation in the C-terminus of the beta-subunit of the
epithelial sodium channel: the Ohasama study. Journal of Hypertension. 2000; 18:861–
866.
39
Matsubara M. Genetic determination of human essential hypertension. Tohoku Journal of
Experimental Medicine. 2000; 192:19–33.
Mattei MG, Hubert C, Alhenc-Gelas F, et al. Angiotensin converting enzyme is on
chromosome 17. Cytogenet Cell Genet. 1989; 51:1041.
McGowan CL, Visocchi A, Faulkner M, Verduyn R, Rakobowchuk M, Levy AS, McCartney
N, Macdonald MJ. Isometric handgrip training improves local flow-mediated dilation in
medicated hypertensives. European Journal of Applied Physiology. 2006;98:355–362.
Ming J, Xinmin C, Jianfeng H, Jianhua Q, Guozhang L, Jiarui W, et al. Polymorphism of
angiotensin I converting enzyme gene in the older Chinese: linked to ambulatory blood
pressure levels and circadian blood pressure rhythm. International Journal of
Cardiology. 1996:55;33-40.
Mondry A, Loh M, Liu P, et al. Polymorphisms of the insertion/deletion ACE and M235T
AGT genes and hypertension: surprising new findings and meta-analysis of data. BMC
Nephrology. 2005; 6:1.
Montgomery H, Marshall R, Humphries SE. Human gene for physical performance. Nature.
1998;393: 221-2.
Myerson S, Hemingway H, Budget R, et al. Human angiotensin I-converting enzyme gene
and endurance performance. Journal of apllied Physiology. 1999: 87:1313–1316.
Nakamura K, Okamura T, Hayakawa T, et al. The proportion of individuals with obesity-
induced hypertension among total hypertensives in a general Japanese population:
NIPPON DATA 80, 90. European Journal of Epidemiology. 2007; 22:691– 698.
Nakano Y, Oshima T, Hiraga H, Matsuura H, Kajiyama G, Kambe M. DD genotype of the
angiotensin I-converting enzyme gene is a risk factor for early onset of essential
hypertension in Japanese patients. Journal of Laboratory and Clinical Medicine.
1998:131;502-6.
Ned RM, Yesupriya A, Imperatore G, et al. The ACE I/D polymorphism in US adults: limited
evidence of association with hypertension-related traits and sex-specific effects by
race/ethnicity. American Jounal of Hypertension. 2012 Feb;25(2):209-15.
O'Donnell CJ, Lindpainter K, Larson MG. et al. Evidence for association and genetic linkage
of the angiotensin-converting enzyme locus with hypertension and blood pressure in man
but not women in the Framingham Heart Study. Circulation. 1998; 97:1766–1772.
Pate RR, Pratt M, Blair SN, et al. Physical activity and public health. A recommendation from
the Centers for Diseases Control and Prevention and the American College of Sports
Medicine. JAMA. 1995: 273: 402–407.
Perusse L, Tremblay A, Leblanc C, et al. Genetic and environmental influences on level of
habitual physical activity and exercise participation. American Journal of Epidemiology
1989; 129(5), 1012–1022.
Province MA, Boerwinkle E, Chakravarti A, et al. Lack of association of the angiotensinogen-
6 polymorphism with blood pressure levels in the comprehensive NHLBI Family Blood
Pressure Program. National Heart, Lung and Blood Institute. Jounal of Hypertension.
2000 Jul; 18(7):867-76.
Rasyid H, Bakri S, Yusuf I. Angiotensin-converting Enzyme Gene Polymorphisms, Blood
Pressure and Pulse Pressure in Subjects with Essential Hypertension in a South Sulawesi
Indonesian Population. Acta Medica Indonesiana. 2012 Oct;44(4):280-3.

40
Rigat B, Hubert C, Alhenc-Gelas F, et al. An insertion/deletion polymorphism in the
angiotensin 1-converting enzyme gene accounting for half the variance of serum enzyme
levels. The Journal of Clinical of Investation. 1990; 86:1343–1346.
Sagnella GA, Rothwell MJ, Onipinla AK, et al. A population study of ethnic variations in the
angiotensin-converting enzyme I/D polymorphism: relationships with gender,
hypertension and impaired glucose metabolism. Journal of Hypertension. 1999
May;17(5):657-64.
Schjerve IE, Tyldum GA, Tjonna AE, et al. Both aerobic endurance and strength training
programmes improve cardiovascular health in obese adults. Clinical Science.
2008;115:283–293.
Slater CH, Green LW, Vernon SW, et al. Problems in estimating the prevalence of physical
activity from national surveys. Preventive Medicine. 1987: 16: 107-118.
Spirduso WW. Dimensões físicas do envelhecimento. Manole: 2005.
Stassen JA, Wang JG, Ginocchio G, et al. The deletion/insertion polymorphism of the
angiotensin converting enzyme gene and cardiovascular-renal risk. Journal of
Hypertension. 1997; 15:1579–1592.
Sugimoto K, Katsuya T, Ohkubo T, et al. Association between angiotensin II type 1 receptor
gene polymorphism and essential hypertension: the Ohasama Study. Hypertension
Research. 2004 Aug;27(8):551-6.
Troosters T, Gosselink R, Decramer M. Six minute walking distance in healthy elderly
subjects. The European Respiratory Journal. 1999: 14: 270-74.
Tuan NT, Adair LS, Stevens J, Popkin BM. Prediction of hypertension by different
anthropometric indices in adults: the change in estimate approach. Public Health
Nutrition. 2010;13:639–46.
Turner S.T, Boerwinkle E, Sing CF. Context-dependent associations of the ACE I/D
polymorphism with blood pressure. Hypertension. 1999; 34:773-778.
Turner ST, Boerwinkle E, Sing CF. Context-Dependent Associations of the ACE I/D
Polymorphism With Blood Pressure. Hypertension. 1999;34:773-778.
Velez DR, Guruju M, Vinukonda G, et al. Angiotensinogen promoter sequence variants in
essential hypertension. American Jounal of Hypertension. 2006 Dec; 19(12):1278-85.
Wacker MJ, Godard MP, McCabe EH, et al. Sex difference in the association of the
angiotensin converting enzyme I/D polymorphism and body mass index. Medical Science
Monitor. 2008; 14: CR353–CR357.
WHO. Active ageing. A policy framework. A contribution of the World Health Organization
to the Second United Nations World Assembly on Ageing. 2002; Madrid, Spain.
WHO. http://www.who.int/mediacentre/factsheets/fs311/en/index.html (2000, accessed
September 2011).
Williams AG, Rayson MP, Jubb M, et al. The ACE gene and muscle performance. Nature.
2000;403:614.
Winnicki M, Accurso V, Hoffmann M, et al. Physical activity and angiotensin-converting
enzyme gene polymorphism in mild hypertensives. American Journal of Medical
Genetics. Part A 2004; 125A(1), 38–44.

41
Wong WP, Zhao Y, Koh WP. Gene polymorphism in angiotensin-I-converting enzyme and
physical activity among normotensive Chinese. Int J Sport Nutr Exerc Metabolism 2012;
22:192-198.
Woo J, Tang NL, Leung J, Kwok T. The Alu polymorphism of angiotensin I converting
enzyme (ACE) and atherosclerosis, incident chronic diseases and mortality in an elderly
Chinese population. The Journal of Nutrition Health Aging. 2012 Mar;16(3):262-8.
Yoshida K, Ishigami T, Nakazawa I, Ohno A, Tamura K, Fukuoka M, et al. Association of
essential hypertension in elderly Japanese with I/D polymorphism of the angiotensin-
converting enzyme (ACE) gene. Journal Human of Genetics. 2000:45;294-8.
Zhang B, Tanaka H, Shono N, et al. The I allele of the angiotensin-converting enzyme gene is
associated with an increased percentage of slow-twitch type I fibers in human skeletal
muscle. Clinical Genetics. 2003; 63:139-44.
42
CONCLUSÃO GERAL
Nosso estudo forneceu evidências adicionais de que o genótipo DD no
gene da ECA, obesidade, e capacidade de exercício prejudicada podem agir de
forma independente sobre a prevalência de EH em idosos brasileiros fisicamente
independentes. Além disso, observou-se associação positiva entre hipertensão e
genêro feminino apresentando genótipo DD, em homens não houve associação.
Serão necessários mais estudos para determinar prescrições de exercícios
ajustadas para os hipertensos com genótipo DD, de modo a eventualmente reduzir a
inatividade e, consequentemente, a hipertensão, entre estes idosos (Winnicki et al.,
2004). Considerando que pouco se sabe sobre a base genética da hipertensão em
idosos brasileiros, a análise do polimorfismo I/D no gene da ECA de uma amostra
dessa população representa informações importantes sobre hipertensão no Brasil.
43
REFERÊNCIAS BIBLIOGRÁFICAS
1. World Health Organization (WHO). World Health Report 2002: reducing risks,
promoting healthy life. Geneva (Switzerland); 2002.
2. Ferreira SRG, Zanella MT. Sistema renina-angiotensina-aldosterona e nefropatia
diabética. Rev Bra Hiper. 2000; 7(3): 268-274.
3. Williams RR, Hunt SC, Hopkins PN, et al. Tabulations and expectations regarding
the genetics of human hypertension. Kidney Int. 1994;44(suppl):S57- S64.
4. Harrap SB, Clark SA, Fraser R, et al. Effects of sodium intake and aldosterone on the
renal pressure natriuresis. Am J Physiol, 1988;254:F697-F703.
5. Baudin B. Polymorphism in angiotensin II receptor genes and hypertension. Exp
Physiol. 2005;90:277-82.
6. Rigat B, Hubert C, Alhenc-Gelas F, et al. An insertion/deletion polymorphism in the
angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme
levels. J Clin Invest. 1990; 86: 1343-6.
7. Bae Y, Park C, Han J, et al. Interaction between GNB3 C825T and ACE I/D
polymorphisms in essential hypertension in Koreans. Journal of Human Hypertension. 2007
Feb;21(2):159-66.
8. Winnicki M, Accurso V, Hoffmann M, et al. Physical activity and angiotensin-
converting enzyme gene polymorphism in mild hypertensives. American Journal of Medical
Genetics. Part A 2004; 125A(1), 38–44.
9. De Moor MHM, LiuYJ, Boomsma DI, et al. Genomewide association study of
exercise behavior in Dutch and American adults. Medicine and Science in Sports and
Exercise 2009; 41(10), 1887–1895.
10. Fuentes RM, Perola M, Nissinen A, et al. ACE gene and physical activity, blood
pressure, and hypertension: A population study in Finland. Journal of Applied Physiology
2002; 92(6), 2508–2512.
11. Hagberg JM, Ferrell RE, McCole SD, et al. VO2 max is associated with ACE
genotype in postmenopausal women. Journal of Applied Physiology 1998; 85(5), 1842–1846.
12. Hernandez D, De La Rosa A, Barragán A, et al. The ACE/DD genotype is associated
with the extent of exercise-induced left ventricular growth. Journal of the American College
of Cardiology. 2003; 42: 527-532.
13. Dias RG, Pereira AC, Negrão CE, et al. Polimorfismos genéticos determinantes da
performance física em atletas de elite. Revista Brasileira de Medicina do Esporte. 2007; 13:
211-216.
14. Myerson S, Hemingway H, Budget R, et al. Human angiotensin-1 converting enzyme
gene and endurance performance. Journal of Applied Physiology. 1999; 87:1313-1316.
15. Whelton SP, Chin A, Xin X, et al. Effect of aerobic exercise on blood pressure: a
meta-analysis of randomized, controlled trials. Ann Intern Med 2002;136: 493e503.
16. Xi B, Cheng H, Shen Y, et al. Physical activity modifies the associations between
genetic variants and hypertension in the Chinese children. Atherosclerosis 2012; 225(2): 376-
80.
44
17. Gomes BMR and Alves JGB. Prevalência de hipertensão arterial e fatores associados
em estudantes de ensino médio de escolas públicas da Região Metropolitana do Recife,
Pernambuco, Brasil, 2006. Reports in Public Health. 2009;25:375-81.
18. Waitzberg DL. Oral nutrition, enteral and parenteral therapy in clinical practice. 3ª ed.
São Paulo: Atheneu; 2001.
19. Sociedade Brasileira de Cardiologia / Sociedade Brasileira de Hipertensão / Sociedade
Brasileira de Nefrologia. VI Diretrizes Brasileiras de Hipertensão. Arq Bras Cardiol 2010;
95(1 supl.1): 1-51.
20. Dosse C, Cesarino CB, Martin JFV, Castedo MCA. Factors associated to patients'
noncompliancewith hypertension treatment. Latin American Journal of Nursing. 2009;17:201-
6.
21. Salgado CM, Carvalhaes JTA. Hipertensão na infância. JPED. 2003;79:115-24.
22. Higaki J, Baba S, Katsuya T, et al. Deletion allele of angiotensin-converting enzyme
gene increases risk of essential hypertension in Japanese men: the Suita study. Circulation.
2000;101:2060-5.
23. Katsuya T, Iwashima Y, Sugimoto K, et al. Effects of antihypertensive drugs and
gene variants in the renin-angiotensin system. Hypertension Research. 2001;24:463-7.
24. Sato N, Katsuya T, Rakugi H, et al. Association of variants in critical core promoter
element of angiotensinogen gene with increased risk of essential hypertension in Japanese.
Hypertension. 1997;30:321-5.
25. Jain S, Vinukonda G, Fiering SN et al. A haplotype of human angiotensinogen gene
containing –217A increases blood pressure in transgenic mice compared with –217G. Am J
Physiol Regul Integr Comp Physiol. 2008;295:1849-57.
26. Ito M, Oliverio MI, Mannon PJ et al. Regulation of blood pressure by the type 1a
angiotensin II receptor gene. Proc Natl Acad Sci USA. 1995;92:3521-5.
27. Wu CK, Tsai CT, Chang YC et al. Genetic polymorphisms of the angiotensin II type
1 receptor gene and diastolic heart failure. Journal of Hypertension. 2009;27:502-07.
28. Payne J, Montgomery H. The renin-angiotensin system and physical performance.
Biochem Soc Trans. 2003;31:1286-9.
29. Terry SE, Sarah ES, Mickey MM. Cardiovascular Disease, Single Nucleotide
Polymorphisms; and the Renin Angiotensin System: Is There a MicroRNA Connection? Am J
Hypertens. 2010:23/281692
30. Dzau VJ. Circulating versus local renin-angiotensin system in cardiovascular
omeostasis Circulation. 1988;77:I4-13.
31. Myerson SG, Montgomery HE, Whittingham M, et al. Left ventricular hypertrophy
with exercise and ACE gene insertion/deletion polymorphism: a randomized controlled trial
with losartan. Circulation. 2001;103:226-30.
32. Jonsson JR, Game PA, Head RJ, Frewin DB. The expression and localization of the
angiotensin-converting enzyme mRNA in human adipose tissue. Blood Press. 1994;3:72-5.
33. Dragovic T, Minshall R, Jackman HL, et al. Kininase II-type enzymes. Their putative
role in muscle energy metabolism. Diabetes. 1996;45(Suppl1):S34-7.
34. Coates D. The angiotensin converting enzyme (ACE). Int J Biochem Cell Biol.
2003;35:769-73.

45
35. Williams AG, Dhamrait SS, Wootton PT, et al. Bradykinin receptor gene variant and
human physical performance. J Appl Physiol. 2004; 96:938-42.
36. O’Donnell CJ, Lindpaintner K, Larson MG, et al. Evidence for association and genetic
linkage of the angiotensin-converting enzyme locus with hypertension and blood pressure in
men but not women in the Framingham Heart Study. Circulation 1998;97(19):1766-72.
37. Sakuma T, Hirata RD, Hirata MH. Five polymorphisms in gene candidates for
cardiovascular disease in Afro-Brazilian individuals. J Clin Lab Anal 2004;18(6):309-16
38. Sagnella GA, Rothwell MJ, Onipinla AK, et al. A population study of ethnic
variations in the angiotensin-converting enzyme I/D polymorphism: relationships with
gender, hypertension and impaired glucose metabolism. J Hypertens 1999;17(5):657-64.
39. Ned RM, Yesupriya A, Imperatore G, et al. The ACE I/D polymorphism in US adults:
limited evidence of association with hypertension-related traits and sex-specific effects by
race/ethnicity. Am J Hypertens. 2012 Feb;25(2):209-15.
40. Morris BJ, Zee RY, Schrader AP. Different frequencies of angiotensin-converting
enzyme genotypes in older hypertensive Individuals. J. Clin Invest 1994;94(3):1085-9.
41. Inacio J, Goulart Filho LG, Vieira GS. Frequências genotípicas e alélicas do gene do
polimorfismo da ECA I/D na população brasileira. Biosci J 2004;20(1):47-51.
42. Almada BVP, Braun V, Nassur BA, et al. Associação da hipertensão arterial com
polimorfismo da enzima conversora da angiotensina em indivíduos idosos. Rev Bras Clin
Med 2010;8(4):320-2.
43. Negrão CE, Rondon MUPB, Brum PC. Adaptação cardiovascular ao treinamento
físico dinâmico. São Paulo: Atheneu; 1996.
44. Wibom R, Hultman E, Johansson M, et al. Adaptation of mitochondrial ATP
production in human skeletal muscle to endurance training and detraining. J Appl Physiol.
1992;73:2004-10.
45. Poole DC, Mathieu CO. Relationship between fiber capillarization and mitochondrial
volume density in control and trained rat soleus and plantaris muscles. Microcirculation.
1996;3:175-86.
46. Rowell LB, Saltin B, Kiens B, et al. Is peak quadriceps blood flow in humans even
higher during exercise with hypoxemia? Am J Physiol. 1986;251:H1038-H1044.
47. Franchini KGB. Circulações regionais. In: Fisiologia Básica. São Paulo: EDUSP; 1999.
48. Holloszy JO, Coyle EF. Adaptations of skeletal muscle to endurance exercise and their
metabolic consequences. J Appl Physiol. 1984;56:831-8.
49. Bouchard C, An P, Rice T, et al. Familial aggregation of VO(2max) response to
exercise training: results from the HERITAGE Family Study. J Appl Physiol. 1999;87:1003-
8.
50. Watson JD, Crick FM. Molecular structure of nucleic acids: a structure deoxyribose
nucleic acid. Nature.1953;25:737-8.
51. Chinn DJ, White M, Howel D, et al. Factors associated with non-participation in a
physical activity promotion trial. Public Health 2006; 120(4), 309–319.
52. Lauderdale DS, Fabsitz R, Meyer JM, et al. Familial determinants of moderate and
intense physical activity: A twin study. Medicine and Science in Sports and Exercise 1997;
29(8), 1062– 1068.

46
53. Lightfoot JT, Turner MJ, Daves M, et al. Genetic influence on daily wheel running
activity level. Physiological Genomics 2004; 19(3), 270–276.
54. Perusse L, Tremblay A, Leblanc C, et al. Genetic and environmental influences on
level of habitual physical activity and exercise participation. American Journal of
Epidemiology 1989; 129(5), 1012–1022.
55. Simonen RL, Rankinen T, Perusse L, et al. Genome-wide linkage scan for physical
activity levels in the Quebec Family study. Medicine and Science in Sports and Exercise
2003; 35(8), 1355–1359.
56. Rankinen T, Perusse L, Rauramaa S, et al. The human gene map for performance and
health-related fitness phenotypes. Med Sci Sports Exer. 2001;33:855-67.
57. Montgomery H, Marshall R, Humphries SE. Human gene for physical performance.
Nature. 1998;393: 221-2.
58. Williams AG, Rayson MP, Jubb M, et al. The ACE gene and muscle performance.
Nature. 2000;403:614.
59. Zhao G, Bernstein RD, Hintze TH. Nitric oxide and oxygen utilization: exercise, heart
failure and diabetes. Coron Artery Dis. 1999;10:315-20.
60. Zhang B, Tanaka H, Shono N, et al. The I allele of the angiotensin-converting enzyme
gene is associated with an increased percentage of slow-twitch type I fibers in human skeletal
muscle. Clin Genet. 2003; 63:139-44.
61. Nazarov IB, Woods DR, Monthomery HE, et al. Th e angiotensin converting enzyme
I/D polymorphism in Russian athletes. Eur J Hum Genet 2001; 9: 797-801.
62. Woods D, Hickman M, Jamshidi Y, et al. Elite swimmers and the D allele of the ACE
I/D polymorphism. Hum Genet 2001; 108: 230-232.
63. Hyeon JK, Chul HK, Dong SP, et al. The Impacts of ACE Activity according to ACE
I/D Polymorphisms on Muscular Functions of People Aged 65. Ann Rehabil Med 2012; 36:
433-446.
64. Greenlund LJ, Nair KS. Sarcopenia-consequences, mechanisms, and potential
therapies. Mech Ageing Dev 2003; 124: 287-299.
65. Nair KS. Aging muscle. Am J Clin Nutr 2005; 81: 953-963.
66. Vigano A, Trutschnigg B, Kilgour RD, et al. Relationship between angiotensin-
converting enzyme gene polymorphism and body composition, functional performance, and
blood biomarkers in advanced cancer patients. Clin Cancer Res 2009; 15: 2442-2447.
67. Sanders PM, Russell ST, Tisdale MJ. Angiotensin II directly induces muscle protein
catabolism through the ubiquitin-proteasome proteolytic pathway and may play a role in
cancer cachexia. Br J Cancer 2005; 22: 425-434.
68. Sumukadas D, Struthers AD, McMurdo ME. Sarcopenia- a potential target for
Angiotensin-converting enzyme inhibition? Gerontology 2006; 52: 237-242.
69. Wallace JP. Exercise in Hypertension. Sports Med. 2003;33(8):585-98.
70. Wong WP, Zhao Y, Koh WP. Gene polymorphism in angiotensin-I-converting
enzyme and physical activity among normotensive Chinese. Int J Sport Nutr Exerc
Metabolism 2012; 22:192-198.

47
ANEXOS
48
ANEXO A
49
50

51
ANEXO C
52
53
54

55

56
57
58

59

60